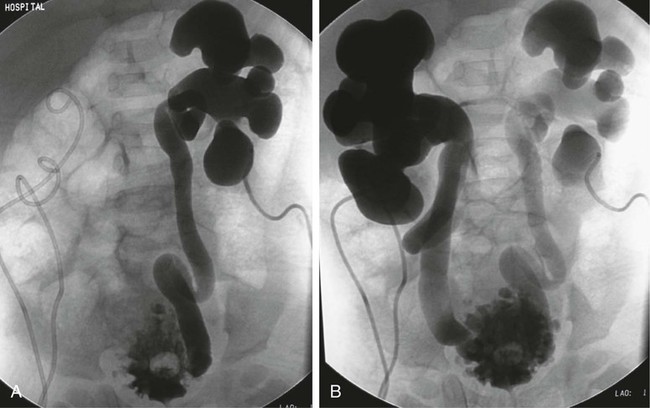
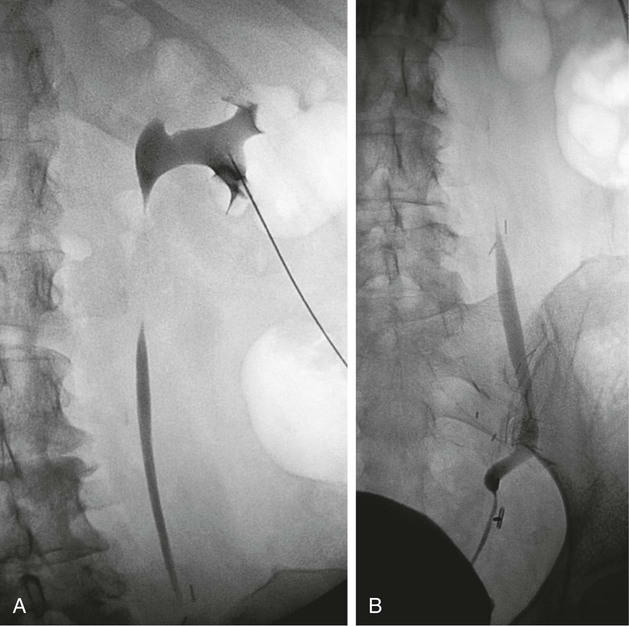
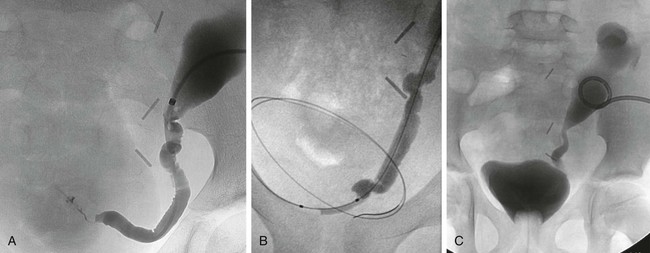
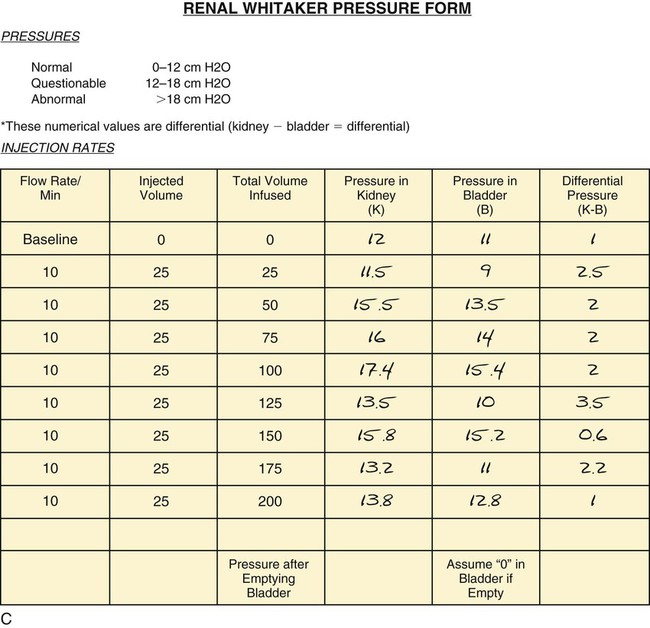
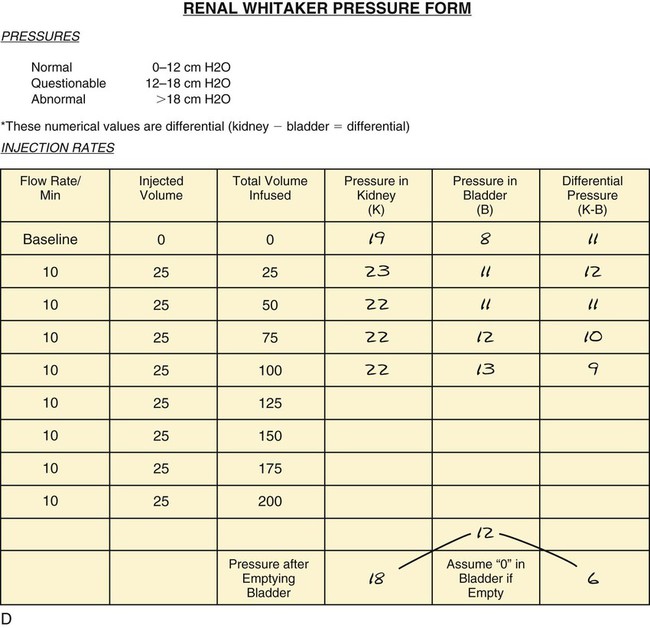
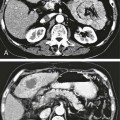
Chapter 145 Causes of nonobstructive dilatation of the renal collecting system include vesicoureteral reflux, urinary tract infection, previous obstruction, congenital malformations, and a noncompliant bladder. Distinguishing between obstructive hydronephrosis and nonobstructive dilatation presents a problem in a number of clinical scenarios. Anatomic evaluation by means such as ultrasonography measures the degree of dilatation but does not delineate the degree of obstruction. Often, this differentiation can be made using radiologic tests such as diuretic renography and intravenous urography, as well as retrograde pyelography. However, these tests sometimes fail to conclusively determine whether an anatomic obstruction exists. It is in such cases that urodynamics can prove most useful.1 • Congenital megaureter—obstructed or nonobstructed?2,3 • Congenital ureteropelvic junction obstruction—severe enough to require surgical repair?5,6 • Any congenital hydronephrosis requiring assessment for obstruction (Fig. 145-1) • Postoperative ureteropelvic junction repair. Is the urine draining well antegrade through the repair? This is often difficult to assess because the renal pelvis will remain large and baggy owing to the previous chronic obstruction.7,8 • Postoperative distal ureteral reimplantation. This also may be difficult to assess if the upper collecting systems remain large or dilated from previous obstruction. • Postoperative balloon dilatation of urinary stricture • Assessment of ureteral strictures after injury, either traumatic or surgical (Fig. 145-2) • Assessment of malignant obstruction resolution after chemotherapy or irradiation • Transplant kidneys with question of obstruction (Fig. 145-3)9–11 • Equivocal results from less invasive tests12 • Suspected obstruction in presence of poor ipsilateral renal function12 • Continued loin pain with upper urinary tract dilatation and a nonobstructive diuresis renogram12 • Unexplained loin pain that might be due to intermittent obstruction at high urine flow rates12 • Definitive investigation of the grossly dilated upper urinary tract where there is concern about the implications of an obstructive diuresis renogram with minimal symptoms12
Urodynamics
Indications
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine