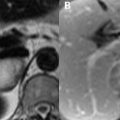
75 Uterine and Cervical Cancer Endometrial carcinoma is predisposed by the development of endometrial hyperplasia and polyps, MRI being of little utility in distinguishing benign and malignant varieties of the latter. Both benign and malignant polyps are of variable SI, the latter identifiable only by myometrial invasion. Submucosal fibroids may appear similar but arise from the myometrium and display uniformly low SI unless degenerative. MRI may be performed if ultrasonographic evaluation of endometrial hyperplasia is not possible. Normal myometrial thickness is less than 5 mm in postmenopausal women and 8 mm in the proliferative (16 mm secretory) phase of premenopausal women. Cystically dilated high SI glandular structures on T2WI are often present in hyperplastic endometrium and do not typically enhance. Findings of endometrial hyperplasia are indistinguishable from those of endometrial carcinoma on MRI with only myometrial invasion proving the latter—the most common invasive carcinoma of the female genital tract. Treatment is guided by grade, but early staging is performed with MRI due to accurate depiction of zonal anatomy on T2WI. Stage 1A lesions, as in Fig. 75.1, are manifest as endometrial thickening without junctional zone disruption. On (A) coronal T2WI, a low SI lesion (white arrow) involves the right side of the endometrium. A hypointense lesion is present on (B) axial T1WI without depiction of the zonal anatomy. The junctional zone, disrupted in 1B lesions, in the (A
![]()
Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


