19
Vascular Anatomy below the Diaphragm
This chapter discusses the relevant anatomy of the abdominal aorta, from the diaphragm to the distal vessels in the foot. Mention is made of important variant anatomy as well as collateral pathways. Detailed variant anatomy and collateral flow patterns are beyond the scope of this text.
 Abdominal Aorta (Fig. 19-1A)
Abdominal Aorta (Fig. 19-1A)
Inferior phrenic
The paired phrenic arteries usually arise from the aorta in close proximity to the aortic hiatus. The inferior phrenic supplies the abdominal surface of the diaphragm. In addition to arising directly from the aorta, it may arise from the celiac artery, its branches or, rarely, from the renal arteries.
Celiac artery (Fig.19-1B)
The celiac artery arises ventrally from the abdominal aorta at the T12–L1 level. The typical branching pattern, seen in approximately 75% of individuals, is the left gastric, common hepatic and splenic arteries. In the remaining individuals, there not be less than a true trifurcation, with aberrant origin of the left gastric or the hepatic arteries. The left gastric artery gives off branches to the distal esophagus and gastric cardia. Branches also supply the lesser curvature of the stomach. The hepatic artery resides in the hepatoduodenal ligament and typically divides into right, middle, and left branches. In about 10% of the population, the right hepatic artery arises from the superior mesenteric artery and is termed a replaced right hepatic artery. Less common variants are origin of the left gastric from the left hepatic artery, which is termed a replaced left gastric artery and left hepatic off the left gastric artery, a replaced left hepatic artery. The cystic artery is most frequently a branch of the right hepatic artery. The right gastric artery is a small vessel that is seldom visualized without selective catheterization. The gastroduodenal artery arises from the common hepatic artery in about three quarters of the population. It gives rise to anterior and posterior superior pancreaticoduodenal arteries and the right gastroepiploic artery. The splenic artery is typically a tortuous vessel with a relatively long course to supply the spleen. The main branches are pancreatic, short gastric, and left gastroepiploic arteries. The splenic artery ultimately ramifies into segmental branches at or within the splenic parenchyma. Major pancreatic branches arise from the splenic artery.
Superior mesenteric artery (Fig.19-1C)
The superior mesenteric artery (SMA) supplies the midgut from the ligament of Treitz to the midtransverse colon. It typically arises about L-1. The origin is just caudal to the celiac artery origin. The first branch is the inferior pancreaticoduodenal artery, which divides and a branch anastomosis with the similarly named superior counterpart to form the pancreaticoduodenal arcades. Vessels found on the left side of the SMA are usually jejunal and ileal branches. The branches terminate as straight vessels, vasa recta, close to the serosa of the bowel. These vessels are located on the mesenteric side of the bowel.
The middle colic artery is a moderate-sized vessel that arises from the anterior surface, which divides into right and left branches. Its supply is to the transverse colon. There is typically a terminal branch of the SMA that continues the inferior course of the vessel. The ileocolic typically arises at a 45-degree angle from the main trunk of the SMA and provides flow to the cecum and anastomotic branches to the right colic. Ileal branches and the appendicular artery arise from this vessel as well. The right colic artery arises between the middle and ileo colic origins. Its branches anastomose with both of these vessels. The right colic supplies the right colon and proximal transverse colon.
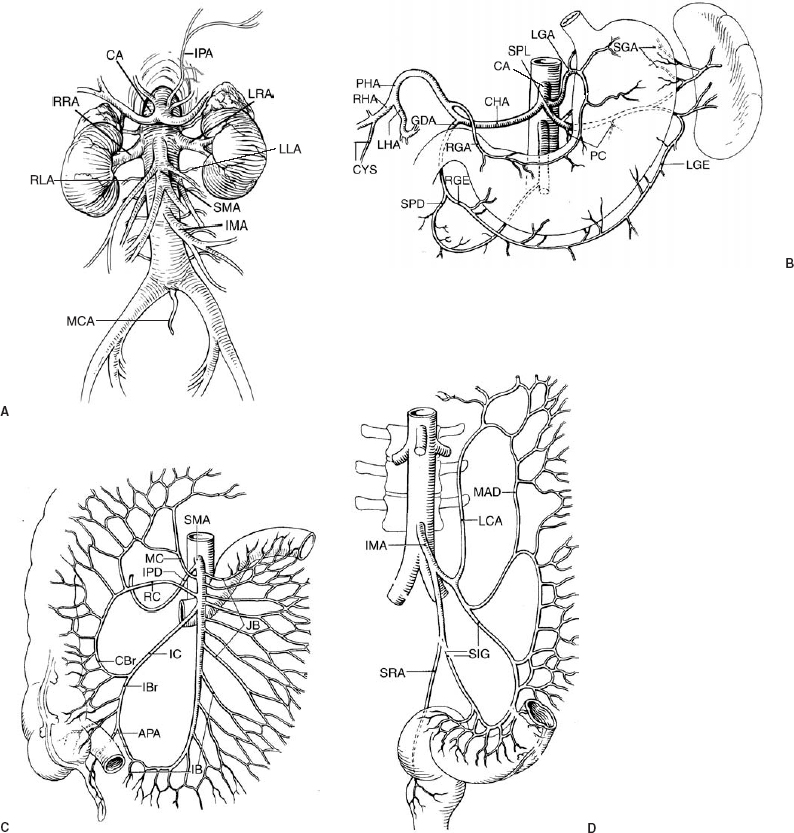
FIGURE 19-1. (A). Abdominal aorta and branches include the inferior phrenic arteries (IPA), celiac artery (CA), superior mesenteric artery (SMA), right and left renal arteries (RRA, LRA), and inferior mesenteric artery (IMA). (B). Celiac artery (CA) and branches include: common hepatic artery (CHA), splenic artery (SPL), left gastric artery (LGA), proper hepatic artery (PHA), right hepatic artery (RHA), left hepatic artery (LHA), cystic artery (CYS), right gastric artery (RGA), gastroduodenal artery (GDA), right gastroepiploic artery (RGE), and superior pancreaticoduodenal artery (SPD). Splenic branches include pancreatic (PC), short gastric artery (SGA), and left gastroepiploic arteries (LGE). (C). Superior mesenteric artery (SMA) and branches include inferior pancreaticoduodenal artery (IPD), jejunal branches (JB), ileal branches (IB), ileocolic artery (IC), right colic artery (RC), middle colic artery (MC). Branches of the ileocolic artery include the appendicular artery (APA), ileal branch (IBr), and colic branch (CBr). (D). Inferior mesenteric artery (IMA) and branches include left colic artery (LCA), sigmoid arteries (SIG), superior rectal artery (SRA), and marginal artery of Drummond (MAD).
Inferior mesenteric artery (Fig. 19-1D)
The inferior mesenteric artery (IMA) arises from the left anterolateral surface of the aorta, on the left at about the L3 level. It supplies the distal transverse colon, left colon, and sigmoid and superior rectum. The left colic is the first branch, which divides into ascending and descending branches. The ascending branch joins the left branch of the middle colic to form the important arc of Riolan. This anastomosis is important because there is a high incidence of IMA origin occlusion in elderly patients. A similar anastomosis is the marginal artery of Drummond. This vessel lies within bowel mesentery and is present along the mesenteric border of the large bowel. The marginal artery of Drummond is formed by the arcades of the ileocolic, right colic, middle colic, and left colic branches. There are usually two or three sigmoid branches arising from the IMA. The final branch of the IMA is the superior hemorrhoidal, which divides to supply both sides of the superior rectum. The superior hemorrhoidal forms an important anastomotic network with middle hemorrhoidal branches. The superior hemorrhoidal is a branch of the internal iliac, and therefore these vascular systems are joined here.
Renal arteries
Related posts:
 Percutaneous Needle Biopsy and Drainage
Percutaneous Needle Biopsy and Drainage
 Arteriography and Venous Sampling of the Parathyroid Glands, Pancreas, and Adrenal Glands
Arteriography and Venous Sampling of the Parathyroid Glands, Pancreas, and Adrenal Glands
 Liver and Spleen
Liver and Spleen
 Anatomy of the Gastrointestinal Tract, Liver, and Biliary System
Anatomy of the Gastrointestinal Tract, Liver, and Biliary System
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


