SPINAL CORD CAVERNOUS MALFORMATION
KEY FACTS
 Histologically, cavernous malformations are composed of dilated vascular sinusoids devoid of smooth muscle and elastic fibers; there are no normal intervening neural tissues, and abundant hemosiderin is present.
Histologically, cavernous malformations are composed of dilated vascular sinusoids devoid of smooth muscle and elastic fibers; there are no normal intervening neural tissues, and abundant hemosiderin is present.
 Cavernous malformations comprise 5% to 10% of spinal vascular malformations but are more common in patients with the syndrome of multiple familial cavernous malformations.
Cavernous malformations comprise 5% to 10% of spinal vascular malformations but are more common in patients with the syndrome of multiple familial cavernous malformations.
 If strictly intramedullary these malformations are usually solitary.
If strictly intramedullary these malformations are usually solitary.
 Common clinical symptoms include progressive paraparesis, sensory alterations, pain, and occasionally subarachnoid hemorrhage or hematomyelia.
Common clinical symptoms include progressive paraparesis, sensory alterations, pain, and occasionally subarachnoid hemorrhage or hematomyelia.
 Main differential diagnosis: arteriovenous malformation (AVM), hemorrhagic tumor (primary or metastases), hemorrhagic contusion.
Main differential diagnosis: arteriovenous malformation (AVM), hemorrhagic tumor (primary or metastases), hemorrhagic contusion.
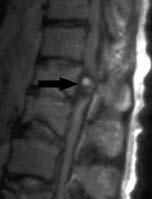
FIGURE 23-1. Midsagittal T2 shows rounded cavernous malformation (arrow) in the distal spinal cord. Note internal mixed signal intensities and surrounding hypointense rim typical of these malformations.
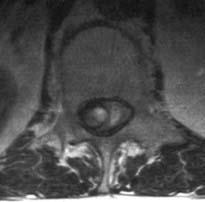
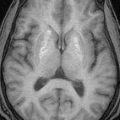
FIGURE 23-2. Axial T2, in the same patient, shows again the features of the lesion located mostly to the right in the canal.

FIGURE 23-3. Midsagittal fat-suppressed post-contrast T1 image shows expanding and enhancing lesion (arrow) at C7.
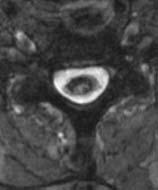
FIGURE 23-4. Axial T2, in the same patient, shows intramedullary lesion with prominent surrounding hemosiderin rim.

FIGURE 23-5. Midsagittal T2, in a different patient, shows the cavernoma in medulla with hemorrhage in the spinal cord.

FIGURE 23-6. Corresponding T1 image clearly shows the typical features of the cavernoma and high signal in hematomyelia.
SUGGESTED READING
Santoro A, Piccirilli M, Frati A, Salvati M, Innocenzi G, Ricci G, et al. Intramedullary spinal cord cavernous malformations: report of ten new cases. Neurosurg Rev 2004;27:93–98.
 SPINAL CORD ARTERIOVENOUS MALFORMATIONS
SPINAL CORD ARTERIOVENOUS MALFORMATIONS
KEY FACTS
 Spinal cord arteriovenous malformations (AVMs) may be of the following types:
Spinal cord arteriovenous malformations (AVMs) may be of the following types:
 Small mass-like vascular nidus (glomus) supplied by multiple feeders from anterior and/or posterior spinal arteries and draining into enlarged veins.
Small mass-like vascular nidus (glomus) supplied by multiple feeders from anterior and/or posterior spinal arteries and draining into enlarged veins.
 Large mass-like vascular nidus with extramedullary extension supplied by a myriad of arterial feeders (juvenile type).
Large mass-like vascular nidus with extramedullary extension supplied by a myriad of arterial feeders (juvenile type).

FIGURE 23-7. Midsagittal T2 shows multiple dilated blood vessels in and outside the distal spinal cord. Fast flow in these vessels results in their signal void.

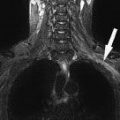
FIGURE 23-8. Coronal T2, in the same patient, shows the large interiorly located vascular nidus with venous “aneurysms.”

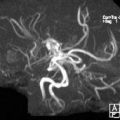
FIGURE 23-9. 3-D DSA, in a different patient, shows large AVM fed vessels arising from multiple intercostals arteries. (Case courtesy J. Ramalho, Lisbon, Portugal.) (See color insert)

FIGURE 23-10. Midsagittal T2 image, in a different patient, shows diffuse cord edema and a focal area of dark signal at C2.
 Large malformation involving the spinal cord and adjacent vertebrae and soft tissues (meta-meric type).
Large malformation involving the spinal cord and adjacent vertebrae and soft tissues (meta-meric type).
 Common locations: cervical, lower thoracic and upper lumbar spine; most are found in middle-aged men.
Common locations: cervical, lower thoracic and upper lumbar spine; most are found in middle-aged men.
 Common symptoms: paresis, sensory alterations, autonomic dysfunction, and impotence.
Common symptoms: paresis, sensory alterations, autonomic dysfunction, and impotence.
 Main differential diagnosis: hypervascular tumor (hemangioblastoma, metastases), cavernous hemangioma.
Main differential diagnosis: hypervascular tumor (hemangioblastoma, metastases), cavernous hemangioma.
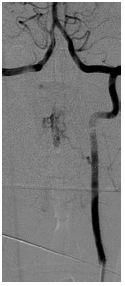
FIGURE 23-11. Frontal DSA view, in the same patient as 23-10, shows AVM fed by a left vertebral artery branch.

FIGURE 23-12. Midsagittal T2 in a child shows abnormal signal in conus and serpiginous appearance of nerve roots.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


