John Reidy, Nigel Hacking and Bruce McLucas (eds.)Medical RadiologyRadiological Interventions in Obstetrics and Gynaecology201410.1007/174_2014_1010
© Springer-Verlag Berlin Heidelberg 2014
Pelvic Venous Congestion
(1)
School of Medicine, University of St Andrews, North Haugh, Fife KY16 9TF, St Andrews, UK
Abstract
Pelvic congestion is a diagnosis now infrequently made by gynecologists as a cause of chronic pelvic pain. Recent literature has been almost exclusively from radiological practice and does not always relate the diagnosis to pain. In this context the concept of pelvic congestion is reviewed from an historical perspective, clinical correlates identified, the pathophysiology discussed, and the place of this diagnosis in modern practice considered.
1 Pelvic Congestion: History of the Concept
Taylor proposed the concept of venous congestion as a cause of chronic pain in the mid-twentieth century (Taylor 1949). Congestion referred to dilatation and sluggish flow in the utero-ovarian veins, but this was not a commonly accepted concept in clinical diagnosis. Using a transcervical approach with injection of contrast medium into the myometrium, Beard and colleagues reported a comparison of radiological appearances of the pelvic veins in women with a range of clinical presentations (Beard et al. 1984). In the radiological literature, pelvic congestion was not exclusively linked to symptoms of pain, but a range of other conditions. In further work, a vasoconstrictor was used to provide evidence for a causal relationship between congestion and pain symptoms. Vasoconstriction in the pelvic veins was associated with symptom relief (Reginald et al. 1987).
Pelvic congestion syndrome is probably best considered in terms of a symptom complex primarily presenting in women in the reproductive age group, whereas endometriosis (at least its symptomatic presentation) is more common in nulliparous women, and childbearing does not appear to afford protection from pelvic congestion, probably the latter condition does not have a hormone-dependent inflammatory basis. However, parity is not a risk factor as has been thought in some literature studies. Typical complaints include a shifting location of pain, deep dyspareunia and postcoital pain, and exacerbation of pain after prolonged standing (Beard et al. 1988). Taylor’s original observations included abnormal ovarian morphology in the presence of venous congestion and it is possible that a basis in ovarian endocrine dysfunction may exist: associated ovarian morphology is characterized by predominantly atretic follicles scattered throughout the stroma, while in contrast to polycystic ovary syndrome the volume of the ovary is normal. The thecal androstenedione response to LH was increased as in polycystic ovarian syndrome, but granulosa cell estradiol production was reduced compared to normal tissue (Gilling-Smith et al. 2000).
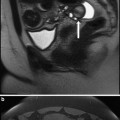
Imaging features of pelvic congestion are dilated uterine and ovarian veins with reduced venous clearance of contrast medium. Ovarian vein reflux seen during transuterine venography was not included as a necessary condition for this diagnosis in the original scoring system, which includes the diameter of the ovarian veins, the distribution of vessels, and delay in clearance of contrast medium. In pregnancy, massively dilated ovarian pelvic veins are seen on ultrasound or visualized at Cesarean section: these are not normally associated with pain probably because these dilated vessels are characterized by high rates of flow.
There is evidence for therapeutic benefit in these patients of reassurance based on the concept of pelvic congestion, thus explanation of their pain in terms of a functional condition similar to cerebral migraine may be appropriate rather than explanations in terms of an anatomical abnormality or progressive pathological condition. Other approaches to therapy have included stress reduction and hormonal therapy with progestogens. Medroxyprogesterone acetate 50 mg as daily dosage has been shown to be effective, (Farquhar et al. 1989) and GnRH agonists with or without estrogen “add-back” are increasingly used in this indication, with some RCT evidence for benefit (Soysal et al. 2001). Hysterectomy and bilateral salpingo-oophorectomy followed by long-term estrogen replacement therapy is an option for those who have extreme symptoms partially or temporarily relieved by hormonal therapy, but this is naturally a treatment of a last resort.
Patients presenting with vulval varices outside of pregnancy, especially those with other sites of peripheral venous disease represent a different clinical entity to “pelvic congestion syndrome” and the underlying disorder may be nonfunctionality of valves in the pelvic veins together with more prominent anastomoses to the ovarian veins. A surgical approach involving extraperitoneal dissection of the ovarian veins has been described for this condition (Hobbs 1976), although details of patient outcomes are lacking in the literature. This is the group of patients that has been evaluated using interventional radiology techniques for vein occlusion in the last 10–15 years. Using percutaneous selective catheterization of the ovarian veins the presence of reflux has been considered diagnostic and to represent an indication for embolotherapy. Selective catheterization studies do not always evaluate the uterine veins and do not include venous clearance of contrast medium in the assessment of congestion, and unfortunately have not always included detailed clinical information. The term “pelvic venous incompetence” has been seen in the literature, emphasizing the presence of “varices” meaning dilated veins, but making no specification regarding reflux or venous clearance (Venbrux et al. 2002). For research and for clinical assessment purposes, it is therefore important to strive for clarity about two possibly distinct conditions as follows:
1.
Women presenting with significant symptoms of pelvic pain and who are found to have ‘pelvic congestion’ including dilated vessels with reduced clearance, but not necessarily ovarian vein reflux. This clinical presentation can be classified as ‘pelvic congestion syndrome’.
2.
Women presenting with vulval varicosities or varices (outside pregnancy) and ovarian vein reflux, with or without pelvic pain.
It is also necessary to consider individuals who are asymptomatic but have either “pelvic congestion” or ovarian vein reflux at venography, MR imaging, or ultrasonography: in this context the imaging findings are likely to be coincidental. Unfortunately, even current reports tend to confuse the diagnostic categories and give incomplete clinical data about the patients included. Van der Vleuten and colleagues report positive outcomes for embolization in “pelvic congestion syndrome” with statistically significant change in summed symptom scores from mean of 26 (on a scale of 10–50) before embolization to 21 two months after the first embolization and to 19 at the time the survey was completed, but do not report detailed symptomatic information, such as presence of dyspareunia or pain scores (van der Vleuten et al. 2012).
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


