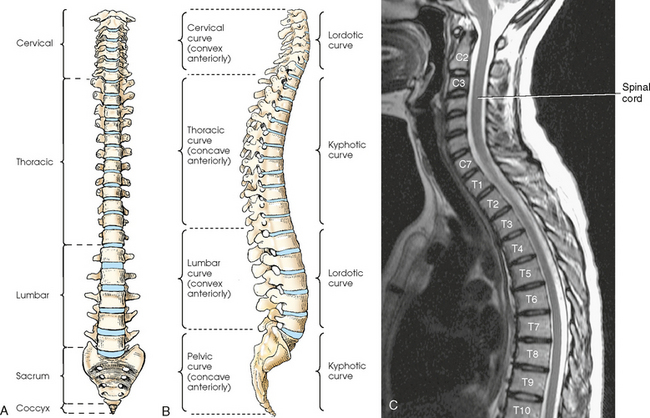
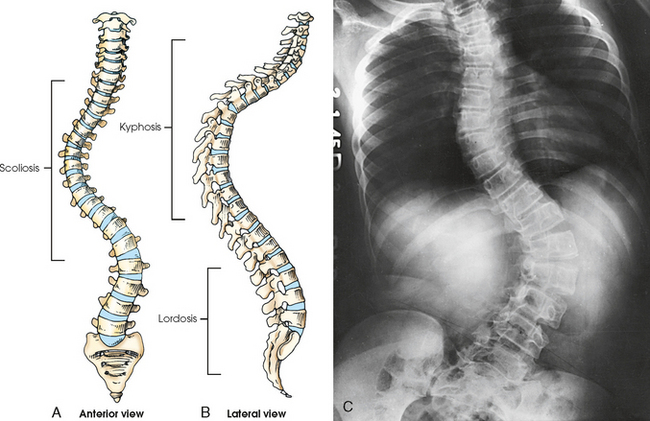
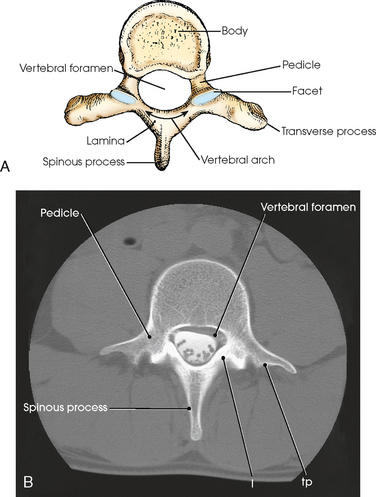
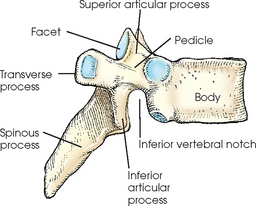
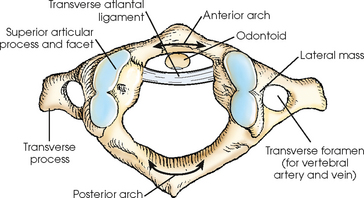
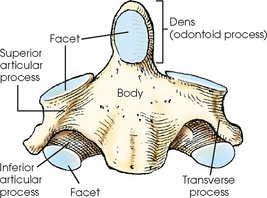
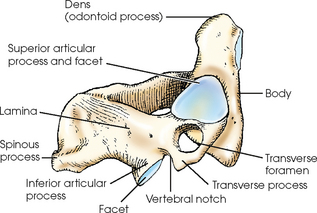
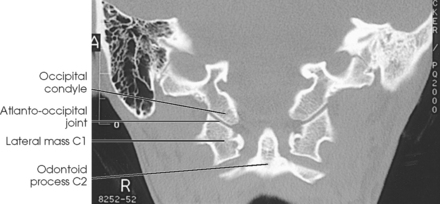
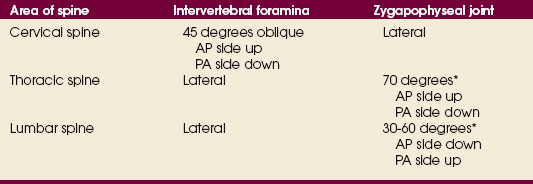
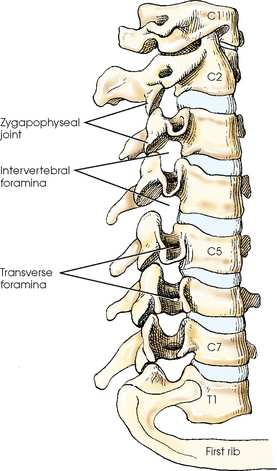
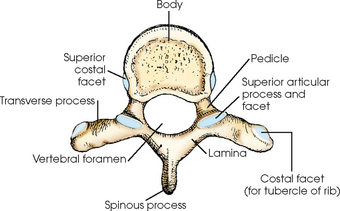
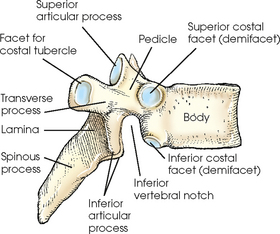
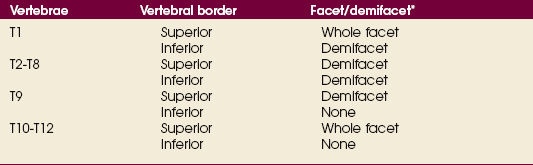
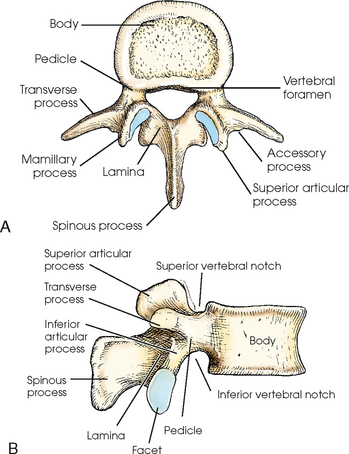
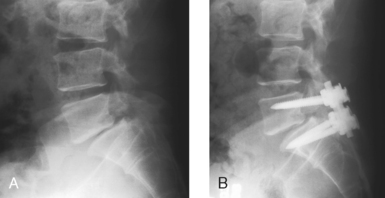
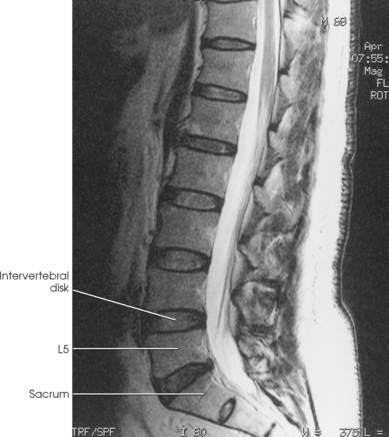
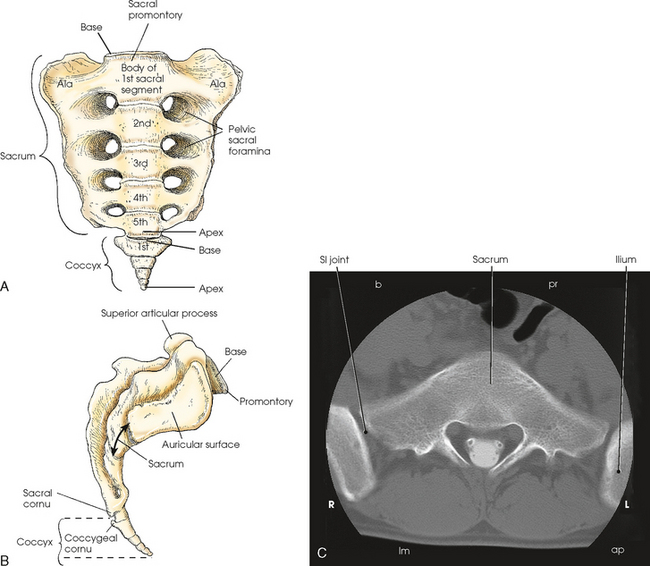
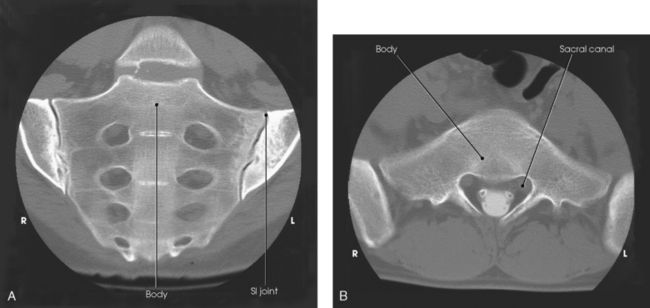
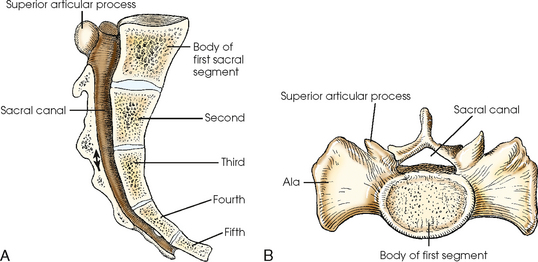
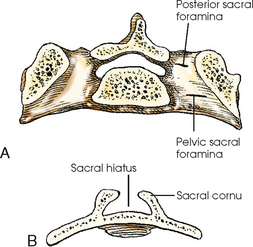
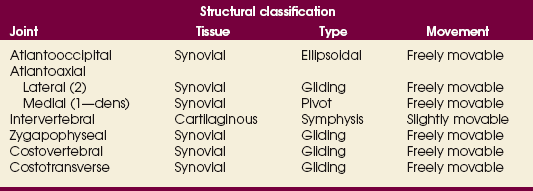
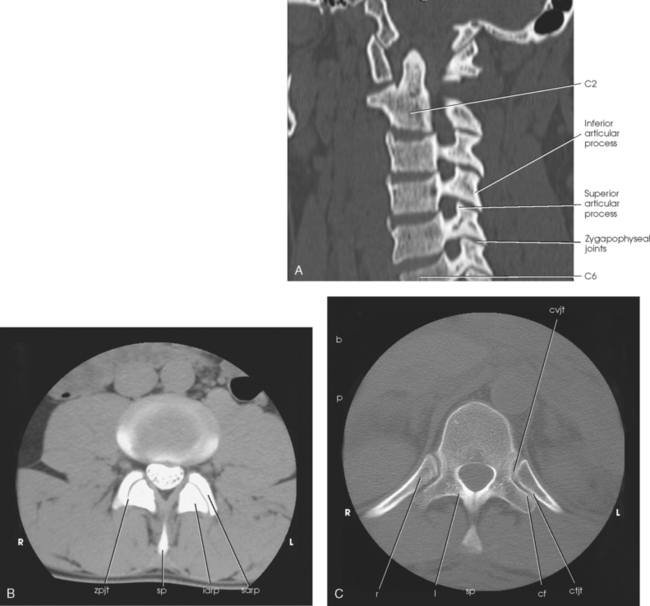
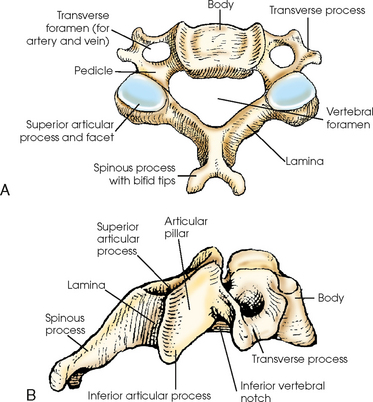
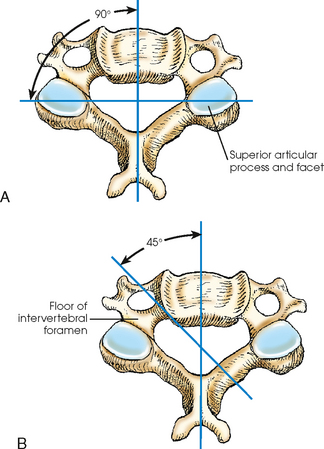
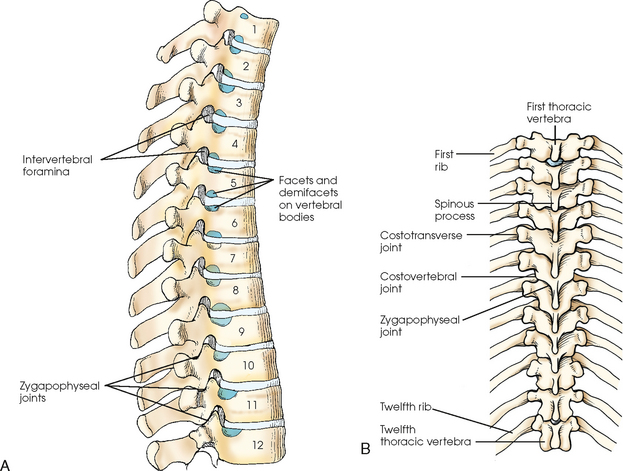
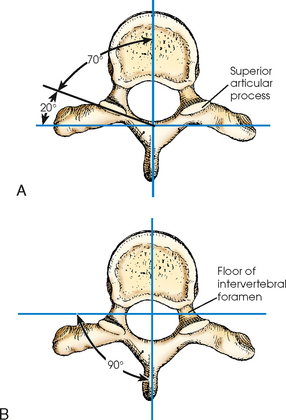
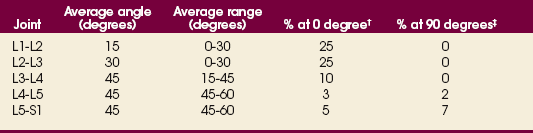
8 In early life, the vertebral column usually consists of 33 small, irregularly shaped bones. These bones are divided into five groups and named according to the region they occupy (Fig. 8-1). The superiormost seven vertebrae occupy the region of the neck and are termed cervical vertebrae. The succeeding 12 bones lie in the dorsal, or posterior, portion of the thorax and are called the thoracic vertebrae. The five vertebrae occupying the region of the loin are termed lumbar vertebrae. The next five vertebrae, located in the pelvic region, are termed sacral vertebrae. The terminal vertebrae, also in the pelvic region, vary from three to five in number in adults and are termed the coccygeal vertebrae. In this text, the vertebral curves are discussed in reference to the anatomic position and are referred to as “convex anteriorly” or “concave anteriorly.” Because physicians and surgeons evaluate the spine from the posterior aspect of the body, convex and concave terminology can be the exact opposites. When viewed posteriorly, the normal lumbar curve can correctly be referred to as “concave posteriorly.” Whether the curve is described as “convex anteriorly” or “concave posteriorly,” the curvature of the patient’s spine is the same. The cervical and lumbar curves, which are convex anteriorly, are called lordotic curves. The thoracic and pelvic curves are concave anteriorly and are called kyphotic curves (see Fig. 8-1 B,). The cervical and thoracic curves merge smoothly. Any abnormal increase in the anterior concavity (or posterior convexity) of the thoracic curve is termed kyphosis (Fig. 8-2, B). Any abnormal increase in the anterior convexity (or posterior concavity) of the lumbar or cervical curve is termed lordosis. In frontal view, the vertebral column varies in width in several regions (see Fig. 8-1). Generally, the width of the spine gradually increases from the second cervical vertebra to the superior part of the sacrum and then decreases sharply. A slight lateral curvature is sometimes present in the upper thoracic region. The curve is to the right in right-handed persons and to the left in left-handed persons. For this reason, lateral curvature of the vertebral column is believed to be the result of muscle action and to be influenced by occupation. An abnormal lateral curvature of the spine is called scoliosis. This condition also causes the vertebrae to rotate toward the concavity. The vertebral column develops a second or compensatory curve in the opposite direction to keep the head centered over the feet (see Fig. 8-2, A). A typical vertebra is composed of two main parts—an anterior mass of bone called the body and a posterior ringlike portion called the vertebral arch (Figs. 8-3 and 8-4). The vertebral body and arch enclose a space called the vertebral foramen. In the articulated column, the vertebral foramina form the vertebral canal. The vertebral arch (see Figs. 8-3 and 8-4) is formed by two pedicles and two laminae that support four articular processes, two transverse processes, and one spinous process. The pedicles are short, thick processes that project posteriorly, one from each side, from the superior and lateral parts of the posterior surface of the vertebral body. The superior and inferior surfaces of the pedicles, or roots, are concave. These concavities are called vertebral notches. By articulation with the vertebrae above and below, the notches form intervertebral foramina for the transmission of spinal nerves and blood vessels. The broad, flat laminae are directed posteriorly and medially from the pedicles. Four articular processes, two superior and two inferior, arise from the junction of the pedicles and laminae to articulate with the vertebrae above and below (see Fig. 8-4). The articulating surfaces of the four articular processes are covered with fibrocartilage and are called facets. In a typical vertebra, each superior articular process has an articular facet on its posterior surface, and each inferior articular process has an articular facet on the anterior surface. The planes of the facets vary in direction in the different regions of the vertebral column and often vary within the same vertebra. The articulations between the articular processes of the vertebral arches are referred to as zygapophyseal joints. Some texts refer to these joints as interarticular facet joints. The atlas, the first cervical vertebra (C1), is a ringlike structure with no body and a very short spinous process (Fig. 8-5). The atlas consists of an anterior arch, a posterior arch, two lateral masses, and two transverse processes. The anterior and posterior arches extend between the lateral masses. The ring formed by the arches is divided into anterior and posterior portions by a ligament called the transverse atlantal ligament. The anterior portion of the ring receives the dens (odontoid process) of the axis, and the posterior portion transmits the proximal spinal cord. The axis, the second cervical vertebra (C2) (Figs. 8-6 and 8-7), has a strong conical process arising from the upper surface of its body. This process, called the dens or odontoid process, is received into the anterior portion of the atlantal ring to act as the pivot or body for the atlas. At each side of the dens on the superior surface of the vertebral body are the superior articular processes, which are adapted to join with the inferior articular processes of the atlas. These joints, which differ in position and direction from the other cervical zygapophyseal joints, are clearly visualized in an AP projection if the patient is properly positioned. The inferior articular processes of the axis have the same direction as the processes of the succeeding cervical vertebrae. The laminae of the axis are broad and thick. The spinous process is horizontal in position. Fig. 8-8 shows the relationship of C1 and C2 with the occipital condyles. The typical cervical vertebrae (C3-6) have a small, transversely located, oblong body with slightly elongated anteroinferior borders (Fig. 8-9). The result is anteroposterior overlapping of the bodies in the articulated column. The transverse processes of the typical cervical vertebra arise partly from the sides of the body and partly from the vertebral arch. These processes are short and wide, are perforated by the transverse foramina for the transmission of the vertebral artery and vein, and present a deep concavity on their upper surfaces for the passage of the spinal nerves. All cervical vertebrae contain three foramina: the right and left transverse foramina and the vertebral foramen. Fig. 8-9 A, Superior aspect of typical cervical vertebra. B, Lateral aspect of typical cervical vertebra. The superior and inferior articular processes are located posterior to the transverse processes at the point where the pedicles and laminae unite. Together the processes form short, thick columns of bone called articular pillars. The fibrocartilaginous articulating surfaces of the articular pillars contain facets. The zygapophyseal facet joints of the second through seventh cervical vertebrae lie at right angles to the midsagittal plane and are clearly shown in a lateral projection (Fig. 8-10, A). Fig. 8-10 A, Direction of cervical zygapophyseal joints. B, Direction of cervical intervertebral foramina. The intervertebral foramina of the cervical region are directed anteriorly at a 45-degree angle from the midsagittal plane of the body (Fig. 8-11; see Fig. 8-10, B). The foramina are also directed at a 15-degree inferior angle to the horizontal plane of the body. Accurate radiographic demonstration of these foramina requires a 15-degree longitudinal angulation of the central ray and a 45-degree medial rotation of the patient (or a 45-degree medial angulation of the central ray). A lateral projection is necessary to show the cervical zygapophyseal joints. The positioning rotations required for showing the intervertebral foramina and zygapophyseal joints of the cervical spine are summarized in Table 8-1. A full view of the cervical spine is shown in Fig. 8-12 along with surrounding tissues. The bodies of the thoracic vertebrae increase in size from the 1st to the 12th vertebrae. They also vary in form, with the superior thoracic bodies resembling cervical bodies and the inferior thoracic bodies resembling lumbar bodies. The bodies of the typical (third through ninth) thoracic vertebrae are approximately triangular in form (Figs. 8-13 and 8-14). These vertebral bodies are deeper posteriorly than anteriorly, and their posterior surface is concave from side to side. The posterolateral margins of each thoracic body have costal facets for articulation with the heads of the ribs (Fig. 8-15). The body of the first thoracic vertebra presents a whole costal facet near its superior border for articulation with the head of the first rib and presents a demifacet (half-facet) on its inferior border for articulation with the head of the second rib. The bodies of the second through eighth thoracic vertebrae contain demifacets superiorly and inferiorly. The ninth thoracic vertebra has only a superior demifacet. Finally, the 10th, 11th, and 12th thoracic vertebral bodies have a single whole facet at the superior margin for articulation with the 11th and 12th ribs (Table 8-2). Fig. 8-15 Thoracic spine. A, Posterior oblique aspect showing zygapophyseal joints, intervertebral foramina, and facets and demifacets (see Table 8-2). B, Posterior aspect showing attachment of ribs and joints. The transverse processes of the thoracic vertebrae project obliquely, laterally, and posteriorly. With the exception of the 11th and 12th pairs, each process has on the anterior surface of its extremity a small concave facet for articulation with the tubercle of a rib. The laminae are broad and thick, and they overlap the subjacent lamina. The spinous processes are long. From the fifth to the ninth vertebrae, the spinous processes project sharply inferiorly and overlap each other, but they are less vertical above and below this region. The palpable tip of each spinous process of the fifth to ninth thoracic vertebrae corresponds in position to the interspace below the vertebra from which it projects. The zygapophyseal joints of the thoracic region (except the inferior articular processes of the 12th vertebra) angle anteriorly approximately 15 to 20 degrees to form an angle of 70 to 75 degrees (open anteriorly) to the midsagittal plane of the body (Fig. 8-16, A; see Fig. 8-15). To show the zygapophyseal joints of the thoracic region radiographically, the patient’s body must be rotated 70 to 75 degrees from the anatomic position or 15 to 20 degrees from the lateral position. Fig. 8-16 A, Direction of thoracic zygapophyseal joints. B, Direction of thoracic intervertebral foramina. The intervertebral foramina of the thoracic region are perpendicular to the midsagittal plane of the body (see Figs. 8-15 and 8-16, B). These foramina are clearly shown radiographically with the patient in a true lateral position (see Table 8-1). During inspiration, the ribs are elevated. The arms must also be raised enough to elevate the ribs, which otherwise cross the intervertebral foramina. A full view of the thoracic vertebrae is seen in Fig. 8-17 along with surrounding tissues. The lumbar vertebrae have large, bean-shaped bodies that increase in size from the first to the fifth vertebra in this region. The lumbar bodies are deeper anteriorly than posteriorly, and their superior and inferior surfaces are flattened or slightly concave (Fig. 8-18, A). At their posterior surface, these vertebrae are flattened anteriorly to posteriorly, and they are transversely concave. The anterior and lateral surfaces are concave from the top to the bottom (Fig. 8-18, B). The laminae lie posterior to the pedicles and transverse processes. The part of the lamina between the superior and inferior articular processes is called the pars interarticularis (Fig. 8-19). The zygapophyseal joints of the lumbar region (Figs. 8-20 and 8-21, A) are inclined posteriorly from the coronal plane, forming an average angle (open posteriorly) of 30 to 60 degrees to the midsagittal plane of the body. The average angle increases from cephalad to caudad with L1-2 at 15 degrees, L2-3 at 30 degrees, and L3-4 through L5-S1 at 45 degrees. Table 8-3 shows, however, that these joint angles may vary widely at each level. Numerous upper joints have no angle, and many lower joints have an angle of 60 degrees or more. Although the customary 45-degree oblique body position shows most clinically significant lumbar zygapophyseal joints (L3 through S1), 25% of L1-2 and L2-3 joints are shown on an AP projection, and a small percentage of L4-5 and L5-S1 joints are seen on a lateral projection. TABLE 8-3 Lumbar zygapophyseal joint angle* *In relation to the sagittal plane. †Joint space oriented parallel to sagittal plane. ‡Joint space perpendicular to sagittal plane. From Bogduk N, Twomey L: Clinical anatomy of the lumbar spine, ed 3, London, 1997, Churchill Livingstone. The intervertebral foramina of the lumbar region are situated at right angles to the midsagittal plane of the body except for the fifth, which turns slightly anteriorly (Fig. 8-21, B). The superior four pairs of foramina are shown radiographically with the patient in a true lateral position; the last pair requires slight obliquity of the body (see Table 8-1). Spondylolysis is an acquired bony defect occurring in the pars interarticularis, the area of the lamina between the two articular processes. The defect may occur on one or both sides of the vertebra, resulting in a condition termed spondylolisthesis. This condition is characterized by the anterior displacement of one vertebra over another, generally the fifth lumbar over the sacrum. Spondylolisthesis almost exclusively involves the lumbar spine (Fig. 8-22). Spondylolisthesis is of radiologic importance because oblique-position radiographs show the “neck” area of the “Scottie dog” (i.e., the pars interarticularis). (Oblique positions involving the lumbar spine, including the Scottie dog, are presented later in this chapter, starting with Fig. 8-95.) A full view of the lumbar vertebrae is seen in Fig. 8-23 along with surrounding tissues. The sacrum is formed by fusion of the five sacral vertebral segments into a curved, triangular bone (Figs. 8-24 and 8-25). The sacrum is wedged between the iliac bones of the pelvis, with its broad base directed obliquely, superiorly, and anteriorly and its apex directed posteriorly and inferiorly. Although the size and degree of curvature of the sacrum vary considerably in different patients, the bone is normally longer, narrower, more evenly curved, and more vertical in position in males than in females. The female sacrum is more acutely curved, with its greatest curvature in the lower half of the bone; it also lies in a more oblique plane, which results in a sharper angle at the junction of the lumbar and pelvic curves. The superior portion of the first sacral segment remains distinct and resembles the vertebrae of the lumbar region (Fig. 8-26). The superior surface of the base of the sacrum corresponds in size and shape to the inferior surface of the last lumbar segment, with which it articulates to form the lumbosacral junction. The concavities on the upper surface of the pedicles of the first sacral segment and the corresponding concavities on the lower surface of the pedicles of the last lumbar segment form the last pair of intervertebral foramina. The superior articular processes of the first sacral segment articulate with the inferior articular processes of the last lumbar vertebra to form the last pair of zygapophyseal joints. On each side of the sacral base is a large, winglike lateral mass called the ala (see Fig. 8-26, B). At the superoanterior part of the lateral surface of each ala is the auricular surface, a large articular process for articulation with similarly shaped processes on the iliac bones of the pelvis. The inferior surface of the apex of the sacrum (Fig. 8-27) has an oval facet for articulation with the coccyx and the sacral cornua, two processes that project inferiorly from the posterolateral aspect of the last sacral segment to join the coccygeal cornua. The coccyx is composed of three to five (usually four) rudimentary vertebrae that have a tendency to fuse into one bone in the adult (see Fig. 8-24). The coccyx diminishes in size from its base inferiorly to its apex. From its articulation with the sacrum it curves inferiorly and anteriorly, often deviating from the midline of the body. The coccygeal cornua project superiorly from the posterolateral aspect of the first coccygeal segment to join the sacral cornua. The joints of the vertebral column are shown in Fig. 8-28 and summarized in Table 8-4. A detailed description follows. The vertebral articulations consist of two types of joints: (1) intervertebral joints, which are between the two vertebral bodies and are cartilaginous symphysis joints that permit only slight movement of individual vertebrae but considerable motility for the column as a whole, and (2) zygapophyseal joints, which are between the articulation processes of the vertebral arches and are synovial gliding joints that permit free movement (see Fig. 8-20). The movements permitted in the vertebral column by the combined action of the joints are flexion, extension, lateral flexion, and rotation. The articulations between the atlas and the occipital bone are synovial ellipsoidal joints and are called the atlantooccipital articulations (see Fig. 8-8). The anterior arch of the atlas rotates around the dens of the axis to form the atlantoaxial joint, which is a synovial gliding articulation and a synovial pivot articulation (see Table 8-4). In the thoracic region, the heads of the ribs articulate with the bodies of the vertebrae to form the costovertebral joints, which are synovial gliding articulations. The tubercles of the ribs and the transverse processes of the thoracic vertebrae articulate to form costotransverse joints, which are also synovial gliding articulations (see Fig. 8-15). The articulations between the sacrum and the two ilia—the sacroiliac joints—(see Fig. 8-25, A) are discussed in Chapter 7.
VERTEBRAL COLUMN

Vertebral Column
Vertebral Curvature
Typical Vertebra
Cervical Vertebrae
ATLAS
AXIS
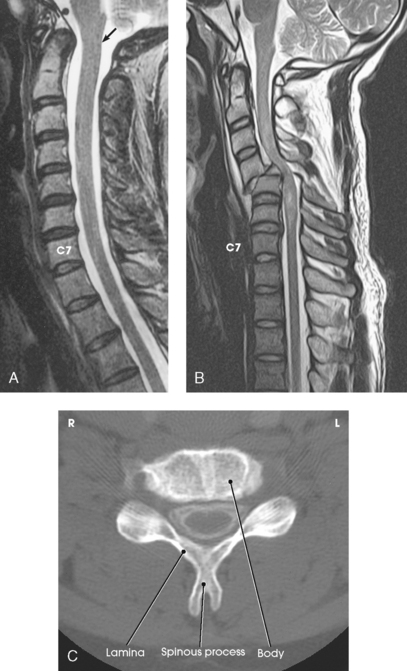
TYPICAL CERVICAL VERTEBRA
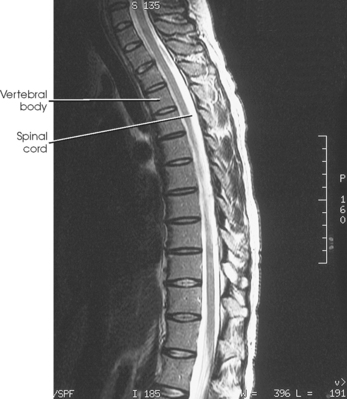
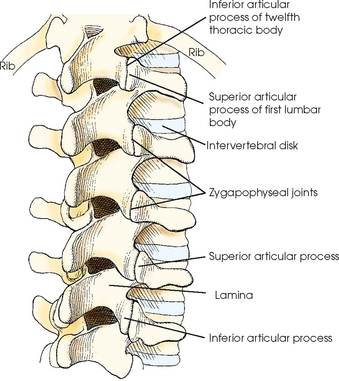
Thoracic Vertebrae
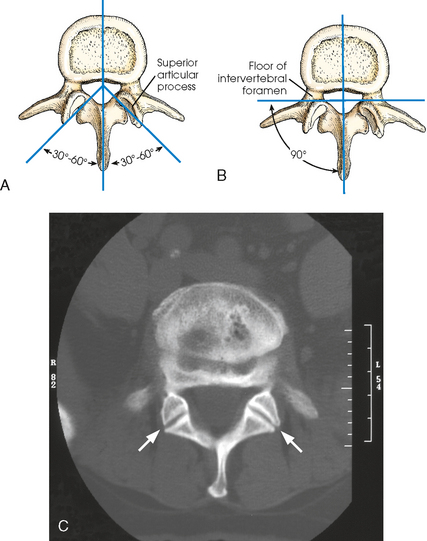
Lumbar Vertebrae
Sacrum
Coccyx
Vertebral Articulations