Viral Pneumonia
Jud W. Gurney, MD, FACR
Key Facts
Terminology
Pulmonary infection with viral pathogen typically affects respiratory epithelium from trachea to terminal bronchioles
Pneumonic (alveolar involvement) less common but often severe and rapidly progressive
Imaging Findings
Centrilobular nodules 4-10 mm in diameter and ground-glass opacities in peribronchial distribution
Course
Insidious: Tracheobronchitis, typically slow development over 7-14 days
Fulminant: Pulmonic pattern, typically rapid progression disease from noncardiogenic edema or hemorrhage
Late: Bronchiolitis obliterans due to damage of small airways
Bacterial superinfection, consider if sudden worsening, development of cavitation, or enlarging pleural effusion
Top Differential Diagnoses
Hypersensitivity Pneumonitis
Bacterial Pneumonia
Mycobacterial Avium Complex
Pathology
Portal of entry
Inhalation droplets or contact with contaminated surfaces (droplets may remain viable for 24-48 hours)
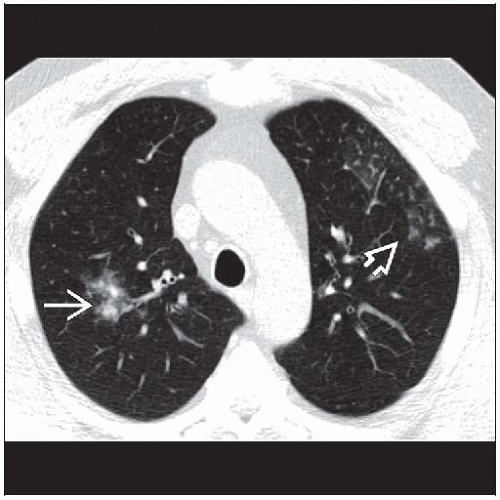 Axial NECT shows centrilobular nodules  with indistinct ground-glass edges. Note the faint tree-in-bud opacities in the left upper lobe with indistinct ground-glass edges. Note the faint tree-in-bud opacities in the left upper lobe  . . |
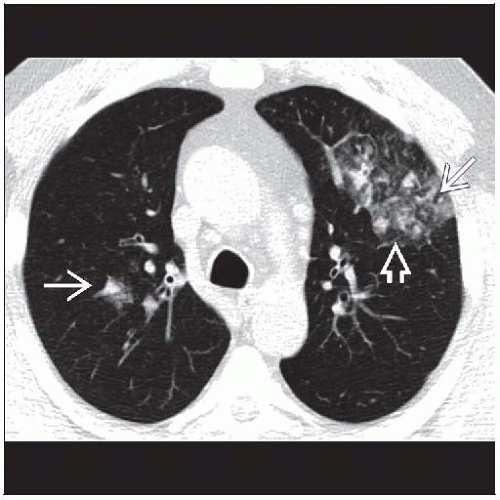 Axial NECT shows centrilobular nodules  admixed with ground-glass opacities admixed with ground-glass opacities  in this patient with community-acquired pneumonia from viral pneumonia. in this patient with community-acquired pneumonia from viral pneumonia. |
TERMINOLOGY
Abbreviations and Synonyms
Cytomegalovirus (CMV), severe acute respiratory syndrome (SARS), Epstein-Barr virus (EBV)
Definitions
Pulmonary infection with viral pathogen, typically affects respiratory epithelium from trachea to terminal bronchioles
Pneumonic (alveolar involvement) less common but often severe and rapidly progressive
IMAGING FINDINGS
General Features
Best diagnostic clue: Centrilobular nodules and ground-glass opacities in peribronchial distribution
Patient position/location: Peribronchial centrilobular nodules
Size: Centrilobular nodules 4-10 mm in diameter
Morphology: Centrilobular nodules in patchy distribution most helpful finding to distinguish infectious vs. noninfectious disease
CT Findings
Variable and nonspecific appearance
Bronchiolitis (small airways involvement)
Centrilobular nodules
4-10 mm in diameter, may be miliary
Patchy peribronchial distribution
Ill-defined edges, may have ground-glass halos
Usually associated with background of ground-glass opacities
Pathologic correlate: Viral involvement of terminal airways
Mosaic attenuation (correlate of hyperinflation)
Tree-in-bud opacities less common than in bacterial pneumonia
Tracheobronchitis (larger airways involvement)
Bronchial wall thickening
Segmental consolidation
Pneumonic (lung involvement)
Consolidation and ground-glass opacities
Pathologic correlate: Noncardiogenic pulmonary edema or diffuse hemorrhage
Distribution: Focal or diffuse
Thickened interlobular septa
Course
Insidious: Slow development over 7-14 days
Primary pattern: Centrilobular nodules
Fulminant: Rapid progressive disease
Primary pattern: Diffuse ground-glass opacities and consolidation
Late: Bronchiolitis obliterans
Pathologic correlate: Healed response to damage of small airways
Uncommon, lung usually returns to normal
Radiographic Findings
Radiography
Variable and overlapping appearance
Tracheobronchitis
Often normal
Segmental opacities (from airway obstruction or pneumonia)
Atelectasis: Discoid to segmental atelectasis (from mucus plugs)
Bronchiolitis
Vague small nodular opacities, patchy distribution
Bronchial wall thickening
Hyperinflation (less common in adults than in children)
Pneumonia
Diffuse consolidation from noncardiac edema or hemorrhage, normal heart size
Pleural effusions, if present, small
Complications
Bacterial superinfection; consider if sudden worsening, development of cavitation, or enlarging pleural effusion
Uncommon findings
Hilar or mediastinal adenopathy: Measles (in children), EBV (infectious mononucleosis)
Splenomegaly
EBV (infectious mononucleosis)
Cardiac enlargement from pericardial effusion
Hantavirus
Pleural effusions
Rare except for adenovirus, measles, hantavirus, herpes simplex type 1
Imaging Recommendations
Best imaging tool
Chest radiography: Usually sufficient for documenting pattern and extent of disease and monitoring therapy
CT: More sensitive; important in immunocompromised patients to document disease and begin early treatment
DIFFERENTIAL DIAGNOSIS
Hypersensitivity Pneumonitis
Farmer’s lung often mistaken for pneumonia: Tends to be recurrent with repeated exposure to offending antigen
May also be febrile
Bacterial Pneumonia
Patchy centrilobular nodules more common in viral or atypical pneumonias
Culture required for management
Mycobacterial Avium Complex
Centrilobular nodules usually associated with ventral bronchiectasisRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



