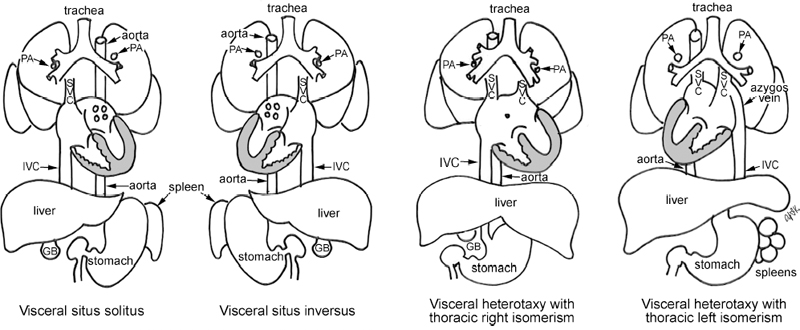
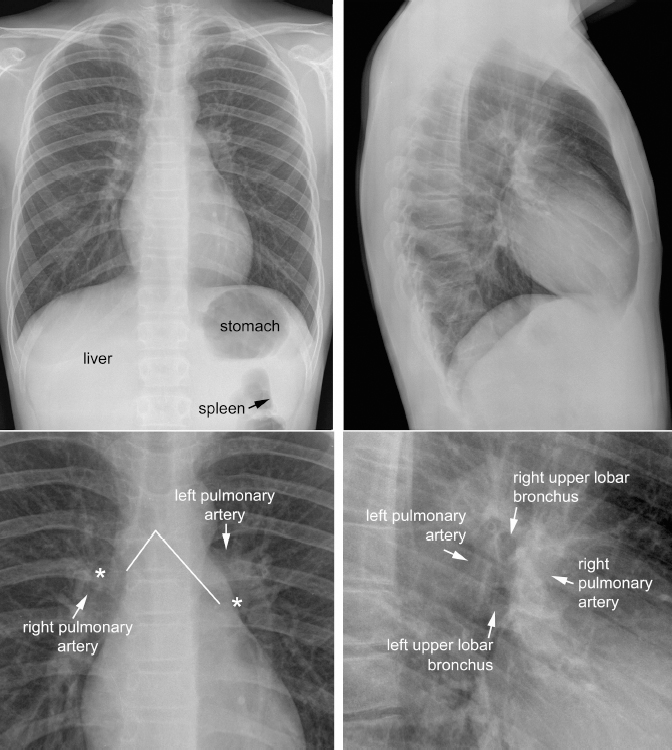
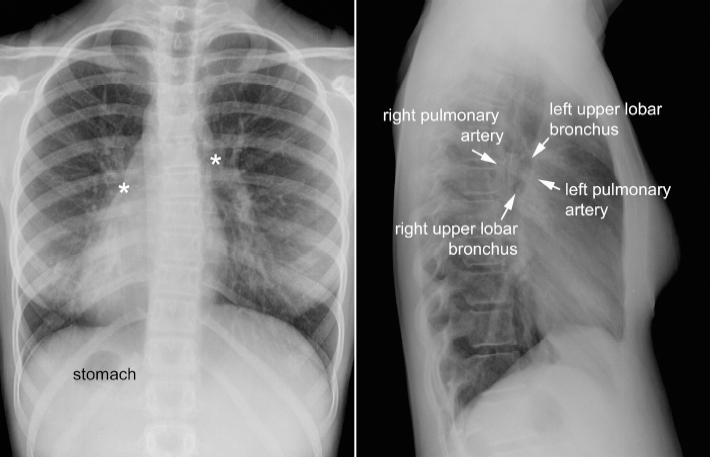
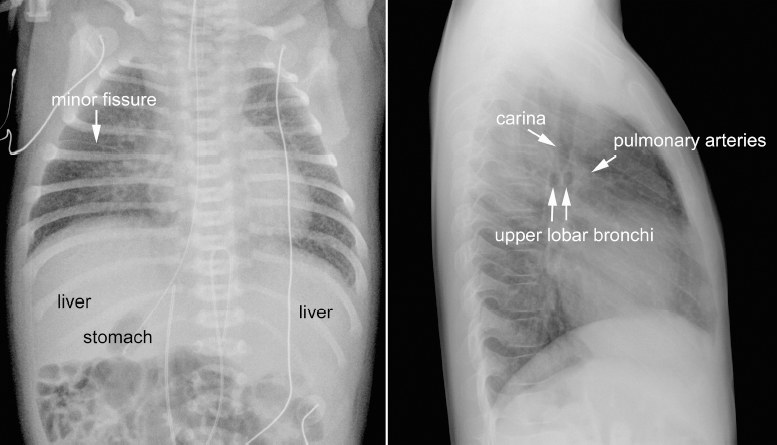
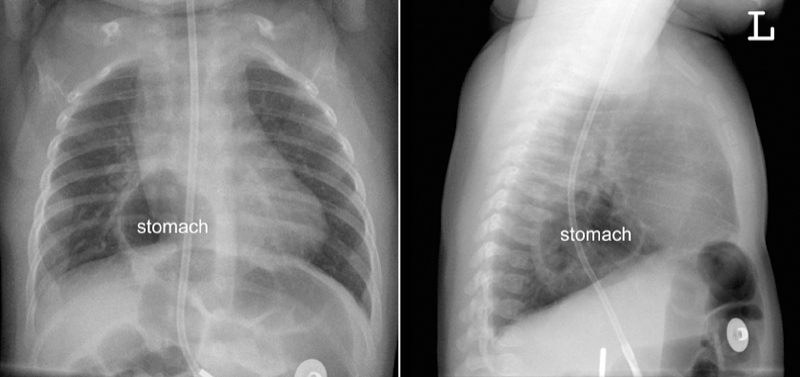
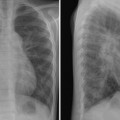
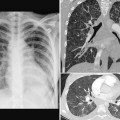
7 Visceral Situs, Heart Position, and Aortic Arch Position The second step in interpretation of a chest radiograph obtained in a new patient is to ascertain visceral situs, the heart position, and the position of the aortic arch relative to the trachea. For example, the radiographic report may start with this sentence: “The radiograph shows situs solitus, levocardia and a left aortic arch.” Visceral situs refers to the pattern of arrangement of the body organs relative to the midline. There are four types of visceral situs: situs solitus, situs inversus, heterotaxy with thoracic right isomerism, and heterotaxy with thoracic left isomerism (Fig. 7.1).1–4 Visceral heterotaxy has also been described as situs ambiguus, which means uncertain situs. This term should be abandoned because the situs is not uncertain but rather needs more words to describe it precisely. The structures that are helpful in determination of the situs include (1) the gastric air bubble, (2) the larger lobe of the liver, (3) the tip of the spleen, (4) the bronchi and pulmonary arteries, (5) the minor fissure, and (6) the azygos vein. The basic concepts regarding visceral situs is discussed in detail in Chapter 2. Fig. 7.1 Four types of visceral situs. GB, gallbladder; IVC, inferior vena cava; PA, pulmonary artery; SVC, superior vena cava. In situs solitus, the gastric air bubble is on the left side, and the larger lobe of the liver is on the right side (Fig. 7.2). The splenic tip can often be identified when the stomach and adjacent bowel loops are filled with air. When the bronchial air column can be traced, an asymmetric bronchial branching pattern with a short right and a long left main bronchus can be appreciated on the frontal radiograph. Normally the left main bronchus is 1.5 to 2 times longer than the right main bronchus. At the pulmonary hilum, the left pulmonary artery is seen slightly higher than the right pulmonary artery. The left pulmonary artery is seen above the left upper lobe bronchus, whereas the right pulmonary artery (in fact, its descending branch) is seen below the right upper lobe bronchus. An asymmetric branching pattern of the bronchi and pulmonary arteries is also evident on the lateral radiograph. As the upper lobe bronchi normally have horizontal courses, they are seen as two round lucencies arranged superoinferiorly in the middle mediastinum. The right upper lobe bronchus is located approximately one vertebral height above the left upper lobe bronchus. The right pulmonary artery lies anterior and slightly inferior to the right upper lobe bronchus. The left pulmonary artery lies posterior and superior to the left upper lobe bronchus. In short, the right upper lobe bronchus lies higher than the left, and the left pulmonary artery lies higher than and posterior to the right pulmonary artery. The minor fissure may cast a horizontal linear shadow over the midzone of a trilobed right lung. Situs inversus is characterized by a mirror-image arrangement of the visceral organs (Fig. 7.3). The gastric bubble is on the right and the larger lobe of the liver on the left. However, it is important to understand that the situs should not be called “situs inversus” solely because of the inverted positions of the gastric bubble and hepatic shadow. Plain film diagnosis of situs inversus can only be made when an inverted bronchial and pulmonary arterial branching pattern is clear. A lateral radiograph is helpful in differentiating the lateralized situs (i.e., situs solitus and inversus) from the symmetric situs (i.e., right isomerism or left isomerism). Normal hilar arrangement of the upper lobe bronchi and branch pulmonary arteries on the lateral view with a right-sided gastric bubble on the frontal view is highly suggestive of situs inversus even if the splenic shadow is not identified. Fig. 7.2 Situs solitus. Magnified views of the hilar anatomy (lower panels). Asterisks on the magnified frontal view mark the upper lobe bronchi. The left main bronchus is twice as long as the right main bronchus in this individual (solid lines). In right isomerism, the hepatic shadow usually extends across the upper abdomen (Fig. 7.4). The gastric bubble can be seen on either side but tends to be closer to the midline. Interestingly, about 15% of patients with right isomerism have a hiatal hernia (Fig. 7.5).5 Hiatal hernia can be regarded as a manifestation of visceral heterotaxy. Bilaterally short bronchi can be appreciated in a well-taken frontal radiograph (Fig. 7.6). However, this feature is often unclear in infants. On the lateral radiograph, the end-on shadows of the upper lobe bronchi are seen at the same or similar horizontal level, and the pulmonary arterial shadow is seen mostly in front of the bronchi (Fig. 7.4). The presence of bilateral minor fissures indicates right isomerism (Fig. 7.7). In fact the diagnosis of right isomerism can be entertained when the minor fissure is present on the same side as the stomach even when a minor fissure is identified only on one side (Fig. 7.4, left panel). This is because the minor fissure and stomach cannot be on the same side in either situs solitus or situs inversus, and no minor fissure is present in either lung in left isomerism. However, a potential pitfall is the presence of an accessory fissure, which can simulate a horizontal fissure (Fig. 7.8).6,7 Right isomerism is associated with complex congenital heart disease in almost all cases. We have not seen any single case of right isomerism without complex congenital heart disease. As pulmonary atresia or stenosis is present in the majority of cases, the pulmonary vascularity is usually reduced (Figs. 7.4, 7.5, 7.6, 7.7). Fig. 7.3 Situs inversus. The frontal view shows mirror-image arrangement of the bronchial and pulmonary arterial trees. Asterisks mark the upper lobe bronchi. The lateral view appears identical to that seen in situs solitus (Fig. 7.2) but note the difference in labeling. This patient had Kartagener’s syndrome with subtle pulmonary infiltrates in the right lower lung. Fig. 7.4 Heterotaxy with thoracic right isomerism. The hepatic silhouette extends symmetrically across the upper abdomen. The stomach with a nasogastric tube in place is on the right side, lying somewhat close to the midline. A minor fissure is visible in the right lung. The presence of a minor fissure on the same side of the stomach is conclusive evidence of right isomerism. On the lateral view, the similar length of the right and left main bronchi results in the upper lobe bronchi being projected at a similar horizontal level. The right and left pulmonary arteries are projected mostly in front of the upper lobe bronchi. Fig. 7.5
 Visceral Situs
Visceral Situs
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel



Full access? Get Clinical Tree


