Fig. 30.1
(a) Dumon Y-Stent. (b) Dumon Y-Stent in the obstructed central airways
Y-Shaped Hybrid Stents
The Dynamic Y-Stent is an anatomically shaped bifurcation stent with an anterolateral silicone wall reinforced with a metallic hoop and a non-reinforced posterior wall resembling the membranous part of the trachea (Figs. 30.2a, b, and 30.3). This flexible posterior membrane mimics the dynamic of the Pars membranacea of the trachea. During coughing, the membrane bulges inward, thereby increasing its efficacy. For sealing fistulas, the Dynamic Y-Stent should be chosen following the placement of an esophageal stent, because the non-reinforced posterior wall presses nicely against the anterior wall of the esophageal stent. Removal of this stent is possible without problems at any time. In 1994, Freitag et al. published the results of a 5-year experience of 135 patients suffering from compression stenoses, strictures, or malacias of the central airways or tracheoesophageal fistulas, who were treated with the dynamic bifurcation airway stent. A stent implantation could be achieved in all patients without any major complication and provided immediate relief of dyspnea in most cases. Three months following stent implantation, 24 patients were still alive with stent in place. Twenty-seven times, a successfully tumor-specific treatment with subsequent reduction of central airway stenosis allowed removal of the stent. Eighty-five patients died with the stent still in place after a mean survival time of 123 days in most cases due to their malignant disease.
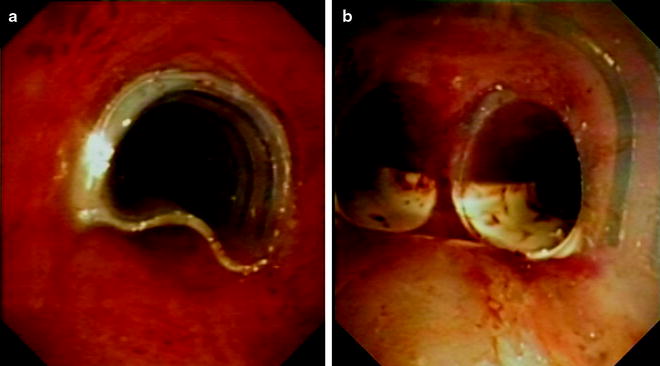
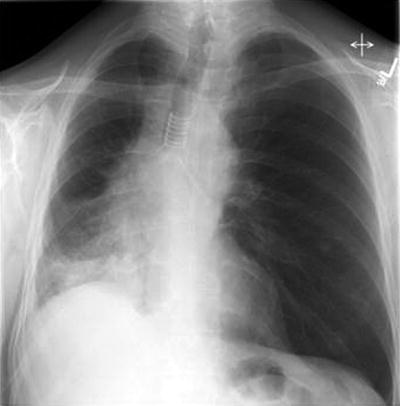
Fig. 30.2
(a) Dynamic Y-stent. Distal end (b) Dynamic Y-stent. Proximal stent
Fig. 30.3
Chest X-ray after implantation of a Dynamic Y-stent
Y-Shaped Metallic Stents
The covered metallic Y-shaped (Fig. 30.4) stents are excellent for use in palliation of airway obstruction. They are easy to place and are characterized by an excellent conformity for irregular tracheal or bronchial walls. Furthermore, problems with retained secretion and mucostasis can be observed.

Fig. 30.4
Self-expandable metallic Y-stent
The bifurcated Nanjing stents also known as Y-Carina-Ecostent are woven metallic stents consisting of highly elastic nitinol wire. They are completely covered expect the distal 5 mm of the right branch. The stents are available in different lengths and diameters. These self-expanding stents are implanted using an introducer system under fluoroscopy. The stent placement is facilitated by radio-opaque markers at different points of the stent. The edges and dinner surface are smooth, but problems like retained secretion has been observed. The disadvantage of the metallic stents is the difficult removal. In 2007, the first clinical results of the implantation of self-expandable metallic Y-stents were published by Yang et al. Five patients with a complex tracheobronchial stenosis due to lung cancer or esophageal cancer were successfully treated with these metallic stents. No procedure-related complications were observed. All patients had immediate relief of respiratory symptoms of dyspnea or cough. In another trial, published in 2008, 35 patients with complex tracheobronchial stenoses involving the carina were treated with a self-expandable metallic Y-stent. Stenosis was caused by lung cancer (n = 25) or esophageal carcinoma (n = 10). In all patients, the delivery of the integrated self-expandable Y-shaped metallic stent in the carinal area was technically successful and well tolerated. All patients had immediate relief of respiratory symptoms. Clinical success was observed in 31 patients (89%) 1–7 days after stent placement, the procedure failed in four patients (11%).
Implantation Techniques
Stent implantation is commonly combined with other endoscopic procedures alleviating the acute airway obstruction. In case of intraluminal tumor growth, laser-assisted resection, electrocautery, or cryodebridement offers removal of neoplastic tissue prior to the stent implantation. In the event of extrabronchial compression, balloon dilatation or bouginage can be used to extend the airway followed by stent implantation for stabilization of the narrowed airways. Prior to the implantation of the stent, the length and diameter of the stent have to be determined. The length of stent should cover the stenosis in both main bronchi as well as in the trachea ≥ 5 mm. The diameter of the stent should greater than the diameter of the remaining stenosis after mechanically treatment or dilatation.
Although, stent implantation is possible using flexible bronchoscope, rigid bronchoscopy remains the preferred method for stent implantation that provides handling potential complications. There are different techniques, the Y-stent can be implanted depending of the type of Y-shaped stent. The most commonly utilized Y-stents are the Dumon Y-Stent, the Dynamic Y-Stent, and the self-expandable metallic Y-stents.
Dumon Y-Stent
The Dumon Y-Stents are the most frequently used stents worldwide. The bifurcated model is the latest development in the Dumon series. These stents are inserted ideally by using the introducer system of a special rigid bronchoscope (Efer, Harrell Universal Bronchoscope) (Fig. 30.5). This bronchoscope features a series of interchangeable tubes of various sizes. Two different implantation techniques can be distinguished. In the “pushing method,” the Y-stent is placed inside the tube of the bronchoscope and then pushed blindly out above the main carina in the trachea. Afterward, the limbs of the Y-stent may have to be twisted and positioned with opened grasping forceps to the carina. In the “pulling method,” the Y-stent is deposited completely in the main bronchus that is most narrowed by the tumor. Afterward, the stent is pulled back using rigid forceps until the shorter bronchial limb slips into the other main bronchus.

Fig. 30.5
Efer bronchoscope with Dumon Y-stent
Dynamic Y-Stent
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


