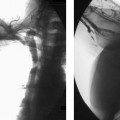
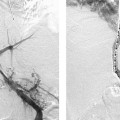
CASE 20 A 41-year-old male presented to the outpatient clinic with intermittent abdominal pain after eating and a 23-pound weight loss over 4 months. Figure 20-1 Diagnosis of median arcuate ligament syndrome. 64-slice multidetector CT angiogram obtained in exhalation shows partial extrinsic compression of the superior aspect of the celiac artery with post-stenotic dilatation. Calcified aortic plaque is present just above the celiac origin. A 64-slice multidetector CT angiogram obtained in exhalation (Fig. 20-1) showed partial extrinsic compression of the superior aspect of the celiac artery with post-stenotic dilatation. Partial obstruction of the celiac artery caused by median arcuate ligament syndrome (MALS). Surgical release of the median arcuate ligament was performed. The patient required no adjunctive treatment to revascularize the celiac artery. MALS describes extrinsic compression of the celiac artery by the median arcuate ligament, or crus, of the diaphragm. Because celiac compression can occur in 5 to 20% of normal individuals, this syndrome is controversial, and clinical information is vital to avoid treating asymptomatic patients. Presentation can include chronic intermittent mild to severe abdominal pain, nausea, diarrhea, and significant weight loss. This syndrome most commonly affects young women (median age, 35 years). Symptoms can be brought on by activities that increase demand and decrease the supply to the mesenteric circulation—including exercise and eating. If left untreated, patients can develop fixed stenoses, aneurysms, or complete occlusion of the celiac artery with development of pancreaticoduodenal collateral pathways to supply the celiac distribution. Aneurysms of pancreaticoduodenal arteries may result, which carry a high risk of rupture. Symptom relief is often achieved by surgical division of the ligament and celiac nerve plexus with revascularization of the celiac artery.
Clinical Presentation

Radiologic Studies
Multidetector CT Angiography
Diagnosis
Treatment
Discussion
Background
Noninvasive Imaging Work-up
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


