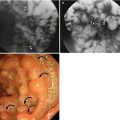
Fig. 18.1
Familial adenomatous polyps. Coronal-reconstructed 2D (a) and surface rendering images (b) of CT colonography (CTC) demonstrate numerous polyps in the entire colon. (c) Circumferential wall thickening at the sigmoid colon (arrow) is noted on coronal 2D image. (d) After total proctocolectomy, tubulovillous adenomas and tubular adenomas are confirmed. Wall thickening at the sigmoid colon was confirmed as ulceroinfiltrative adenocarcinoma (arrow) with moderate differentiation
18.3.2 Hamartomatous Polyps
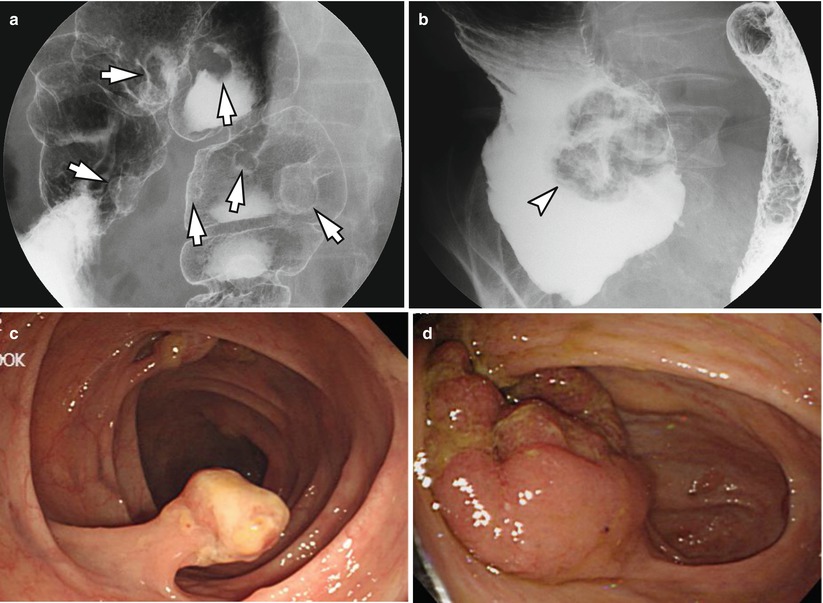
Fig. 18.2
Hamartomatous polyps. (a, b) DCBE reveals multiple pedunculated polyps (arrows) in the transverse and descending colon and a lobulated mass (arrowhead) in the cecum (c, d). Colonoscopy also shows the findings compatible to the images of DCBE. After right hemicolectomy, all the lesions were proved to be hamartomatous polyps with possible differential diagnosis of juvenile polyposis or Cronkhite-Canada syndrome. Some polyps contained adenomatous foci of low grade
18.3.3 Inflammatory Polyps
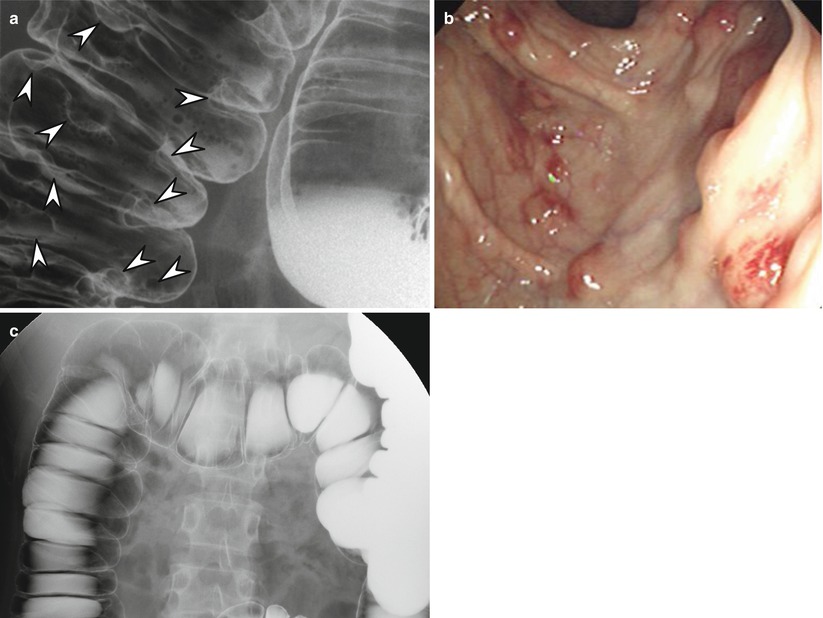
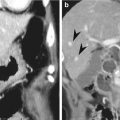
Fig. 18.3
Inflammatory polyps (a) DCBE shows multiple, small, rounding filling defects (arrowheads) mostly in the right colon. (b) Colonoscopy shows multiple polypoid lesions with hemorrhage. The pathologic diagnosis from colonoscopic biopsy from two polyps was granulomatous colitis and chronic colitis. (c) Follow-up DCBE after 8 months shows disappearance of the inflammatory polyps
18.3.4 Differential Diagnosis of a Colonic Diverticulum from a Polyp
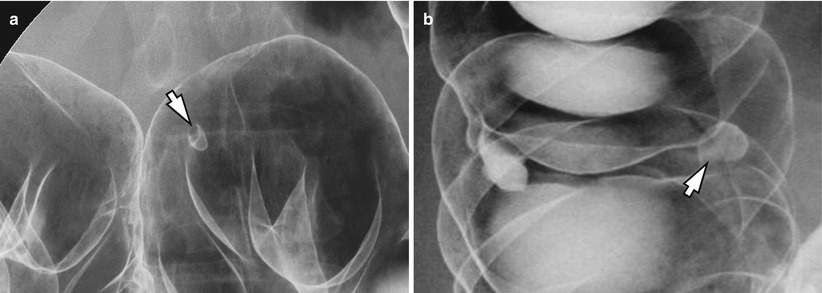
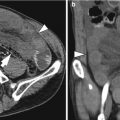
Fig. 18.4
Differential diagnosis of a colonic diverticulum from a polyp with “bowler-hat sign” on DCBE. (a) The dome of a polyp projects toward the lumen (direction of arrow). (b) The dome of a diverticulum projects outward from the wall (direction of arrow)
18.3.5 Diagram Shows the Whole Processes of CT Colonography (CTC)
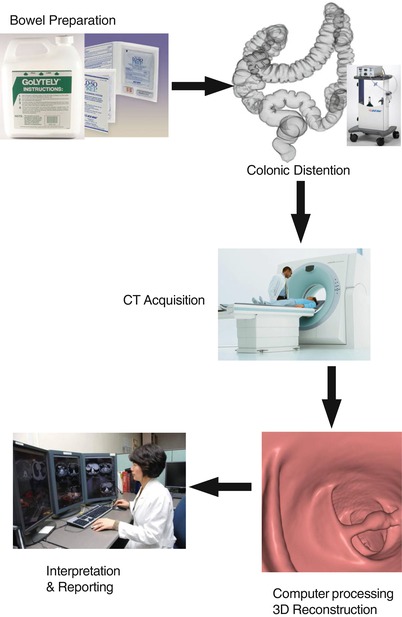
Fig. 18.5
The diagram shows the whole processes of CT colonography
18.3.6 The Importance of Fecal Tagging in CTC
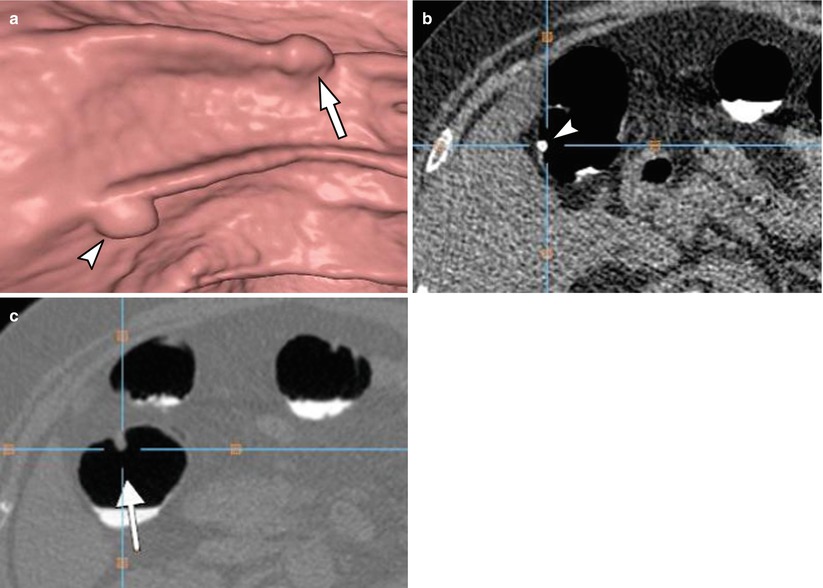
Fig. 18.6
The importance of fecal tagging in CT colonography. (a) A 3D endoluminal image of CT colonography shows two polypoid lesions (arrowhead and arrow) which are similar in appearances. (b) On 2D axial image, the lesion located on the left (arrowhead) on 3D image was shown to be a feces tagged with barium. (c) On 2D axial image, the other lesion on the right (arrow) on 3D image was found to be a true polyp with soft tissue density without fecal tagging
18.3.7 The Importance of Fluid Opacification for CTC
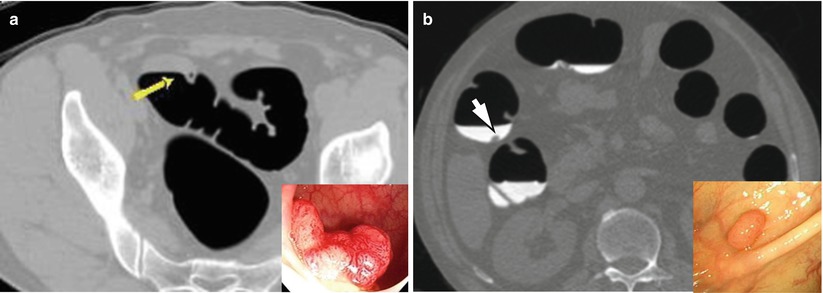
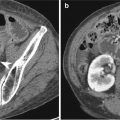
Fig. 18.7
The importance of fluid opacification for CT colonography. (a) 2D image of CT colonography shows fluid without opacification in the sigmoid colon, obscuring a polyp (arrow). A polyp was discovered on colonoscopy (small picture on right lower corner). (b) In another patient, a polyp (arrow) is easily detected within the opacified fluid with water-soluble iodinated contrast material. A small polyp was discovered on colonoscopy (small picture on right lower corner)
18.3.8 The Importance of Colon Distension During CTC
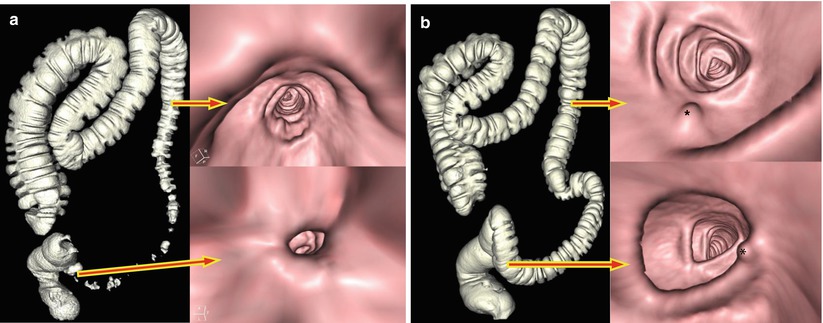
Fig. 18.8
The importance of colon distension during CT colonography. (a) A surface rendering image of CT colonography (left) shows collapse of the descending colon and sigmoid colon. Polyps are not detected at the corresponding segment on endoluminal 3D images (right). (b) In the same patient, two polyps (asterisk) are clearly seen at the proximal descending colon (right upper) and sigmoid colon (right lower) on 3D endoluminal images after adequate distension of the colon. The colon is shown to be well distended on a surface rendering image (left)
18.3.9 The Importance of Dual Positioning During CTC
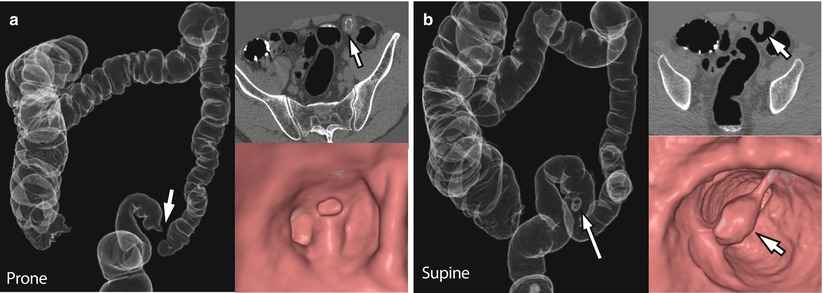
Fig. 18.9




The Importance of dual positioning during CT colonography. (a) On prone position, transparent 3D image of CT colonography (left) shows focal collapse (arrow) of the sigmoid colon. On 2D axial image (right upper), a polypoid lesion (arrow) is suspicious within the collapsed bowel segment, but not shown on endoluminal 3D image (right lower). (b) On supine position, a pedunculated polyp (arrows) on the nondependent bowel wall is unequivocally demonstrated on 2D (right upper) and 3D transparent (left) as well as 3D endoluminal (right lower) images
Related posts:
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
