18 | Doppler Sonography of the Fetal Venous Circulation |
It is known from numerous animal studies on sheep and primate fetuses that the venous circulation, consisting of umbilical v. (UV), ductus venosus (DV), portal v.’s, hepatic v.’s, inferior vena cava (IVC), and the right atrium with the foramen ovale, reflects the central venous pressure and cardiac function. It is also known to play an important role in the regulation of the fetal circulation.
Blood flow in the UV was measured even before the application of Doppler ultrasound in obstetrics in 1980, especially volume flow to monitor fetuses with rhesus incompatibility (Eik-Nes et al. 1980). Subsequent studies concentrated increasingly on the arterial blood vessels of the fetus and on the uterus. Only after the advent of color Doppler ultrasound did it become possible to record the rest of the venous circulation with its narrower vessels and in part very slow blood flow velocities, and to display the anatomical peculiarities of the humans fetus.
Since the beginning of the last decade studies of blood flow in the IVC and the DV were primarily selected for study, but flow in the hepatic v.’s and around the foramen ovale was also studied (Reed et al. 1990, Huisman et al. 1991 and 1992b, Kiserud et al. 1992a, Rizzo et al. 1992, Hecher et al. 1994).
More recently Doppler studies designed to extend our understanding of the fetal circulation in health and disease have also included the conditions of flow in the superior vena cava, the portal v.’s, and the pulmonary v.’s.
Anatomy
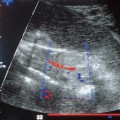
Oxygenated blood from the placenta reaches the body of the fetus through the venous system. The UV enters the fetal abdomen and first runs acutely backward and upward, then divides in the liver into the portal v. (PV) and the DV. From this point, known as the portal sinus, the left PV runs to the right, while the DV runs to the left and in a dorsocranial direction, as it were the continuation of the UV (Fig. 18.1).
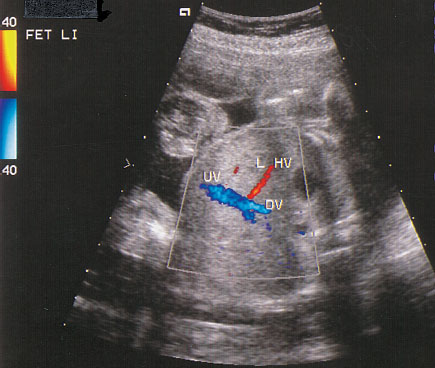
Fig. 18.1 Umbilical vein (UV) and ductus venosus (DV) displayed in a cross section of the fetal abdomen. (LHV = left hepatic vein)
The DV is a trumpet-shaped connection between the UV and the proximal part of the IVC. It is only 2 mm wide at its origin.
The left PV anastomoses with the branches of the right PV, and both supply placental blood to the right lobe of the liver, which receives 80% of the hepatic circulation. The venous drainage takes place through the wide-branching right hepatic v. (RHV) (Fig. 18.2), the main branch of which is the most proximal of the precordial v.’s to drain into the IVC. The UV itself supplies the left lobe of the liver directly with blood which flows into the IVC through the left and middle hepatic v.’s (LHV and MHV).
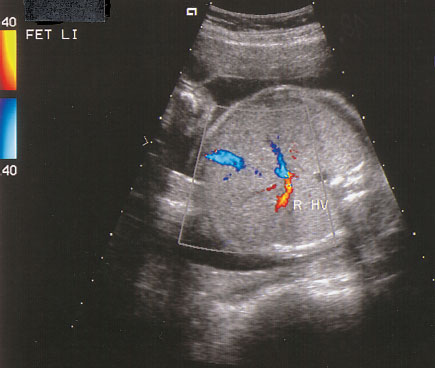
Fig. 18.2 Right hepatic vein (RHV) displayed in a cross section of the fetal abdomen.
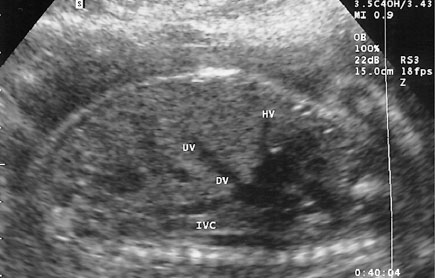
Fig. 18.3 Longitudinal section of the fetal abdomen with display of the junction of the precordial v.’s at the upper portion of the inferior vena cava (IVC). (UV = umbilical vein, DV = ductus venosus, HV = hepatic vein)
The proximal part of the IVC, the DV, and the three hepatic v.’s together form a space situated immediately under the diaphragm before the right atrium, as Huisman et al. (1992a) were able to demonstrate in their anatomical studies. This should be taken into account when the precordial v.’s are examined by Doppler ultrasound, in order to avoid overlapping signals (Fig. 18.3).
Physiology
The DV plays an essential role in the regulation of the fetal circulation. It is one of three shunts and links the UV with the IVC. About 50–60% of the oxygenated blood passes through the DV directly to the fetal heart. The constriction of the lumen of the DV to about a third of the width of the UV and the differences in pressure and resistance in the hepatic and cardiac circulations increase the blood flow velocity from 20 cm/s in the UV to 60–80 cm/s in the DV. Nervous and hormonal influences as well as a sphincter muscle have been suspected of taking part in the regulation of blood flow through the DV, but anatomical correlates for such mechanisms are lacking.
The remaining 40–50% of the blood in the UVs first pass through the PVs into the liver, and then through the hepatic v.’s into the IVC. The oxygen saturation in the UV and the DV is about 80–85 %, while in the distal IVC and the RHV it is only 35% or 50%.
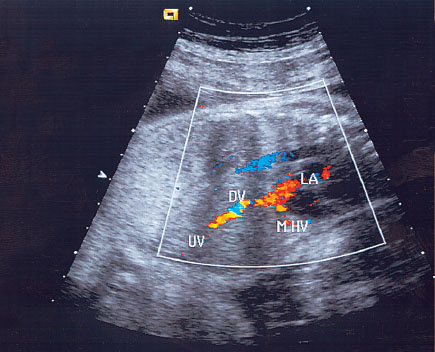
Fig. 18.4 The left path of DV–foramen ovale. (UV = umbilical vein, DV = ductus venosus, MHV = middle hepatic vein, LA = left atrium)
Animal experiments using microspheres carrying radionuclides show two streams of blood, which do not mix, flowing from the proximal IVC to the heart. Kiserud et al. (1992b) used color Doppler ultrasound to show that in the human fetus there are also two crossing inflows to the heart in this area, the left path leading from the DV to the foramen ovale, the right path from the IVC to the right atrium.
The Left Path from the Ductus Venosus to the Foramen Ovale
Well-oxygenated blood from the UV passes through the DV into the left dorsal part of the proximal IVC. The position of the dividing crest of the foramen ovale and the eustachian valve directs this blood flow directly through the foramen ovale into the left atrium. By this route blood rapidly reaches the vital organs, such as brain, heart, and adrenals.
The LHV and MHV, with an oxygen saturation of 70– 75%, also enter this path (Fig. 18.4).
The Right Path from the Inferior Vena Cava to the Right Atrium
The less well oxygenated blood from the lower body and the RHV flows from the anterior right-hand side of the proximal IVC primarily into the right atrium and through the tricuspid valve into the right ventricle. From here it passes through the pulmonary circulation and from there chiefly into the descending thoracic aorta through the ductus arteriosus (Fig. 18.5).
These blood streams effectively do not mix and ensure that the oxygenated blood from the placenta preferentially supplies the small left fetal circulation, while the poorly oxygenated blood from the fetal body returns to the placenta by way of the right heart, the ductus arteriosus, and the aorta.
Related posts:
 Diagnosis of the Uterine Tube by Transvaginal Sonography
Diagnosis of the Uterine Tube by Transvaginal Sonography
 Doppler Sonography in Obstetrics—Screening At-Risk Populations
Doppler Sonography in Obstetrics—Screening At-Risk Populations
 Doppler Ultrasound and the Cardiotocogram
Doppler Ultrasound and the Cardiotocogram
 Doppler Ultrasound in the Diagnosis of Fetal Anomalies
Doppler Ultrasound in the Diagnosis of Fetal Anomalies
 Diagnostic Sonography of Blood Flow in Breast Tumors
Diagnostic Sonography of Blood Flow in Breast Tumors
 Vascular Supply of the Uteroplacentofetal Unit and Techniques for the Examination of Individual Vessels
Vascular Supply of the Uteroplacentofetal Unit and Techniques for the Examination of Individual Vessels
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


