The classification of tendon injuries about the elbow can be organized by location, acuity, and degree of injury. Tendon injury related to a single isolated event is uncommon, although exceptions to this rule do occur. More commonly, tendinous injuries in this location relate to chronic repetitive microtrauma. MRI is particularly well suited, with its excellent soft tissue contrast, to diagnose tendon pathology. This is done primarily by close inspection of signal intensity and morphology of the tendons.
The many muscles and associated tendons of the elbow lend themselves to division into four anatomic regions: posterior, anterior, medial, and lateral. The posterior group includes the triceps and anconeus. The muscles of the anterior group are the biceps brachii and brachialis. The muscles in the medial group are the pronator teres, the palmaris longus, and the flexors of the hand and wrist emanating primarily from the common flexor tendon. The muscles in the lateral group include the supinator, brachioradialis, and extensor muscles of the hand and wrist, the latter arising primarily from the common extensor tendon. Specific anatomic considerations, tendon pathology commonly encountered in the elbow as well as MRI diagnostic criteria are addressed.
Muscle and Tendon Anatomy
Organization of the complex muscular anatomy about the elbow lends itself to division into anterior, posterior, medial, and lateral groups. Although this method allows delineation of the specific muscles and their respective tendons about the elbow, it is important to emphasize that the common flexor and common extensor tendons are involved in the vast majority of musculotendinous pathology about the elbow, thus obviating the need for localizing pathology to a single muscle. To this end, the oblique coronal imaging plane provides optimal visualization of both the common flexor and common extensor tendons, underscoring the importance of obtaining high signal-to-noise ratio fluid-sensitive images in the coronal plane.
The lateral muscle group can be thought of consisting of three components: a superficial group, the common extensors, and the supinator. The superficial group includes the brachioradialis and extensor carpi radialis longus (ECRL). Together with the extensor carpi radialis brevis, the superficial group forms a bulky muscular mass termed the mobile wad, which surrounds much of the anterolateral aspect of the elbow (Fig. 11.1). The brachioradialis forms the most anterior portion of the lateral muscle group, arises from the supracondylar ridge of the humerus, and inserts near the radial styloid process. The extensor carpi radialis longus originates from the supracondylar ridge just distal to the brachioradialis and inserts distally at the base of the second metacarpal.
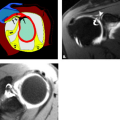
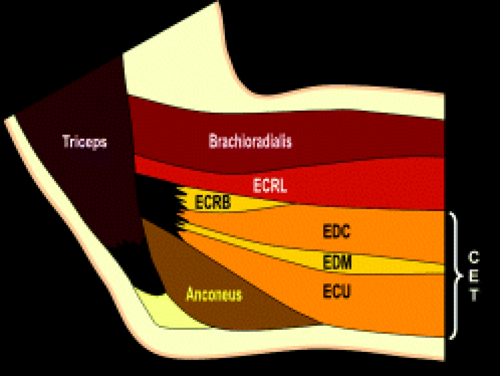 Figure 11.1 Lateral muscle and tendon anatomy. The superficial lateral muscle group consists of the brachioradialis and extensor carpi radialis longus. Together with the extensor carpi radialis, the superficial group forms the muscle mass referred to as the mobile wad. The common extensor group is composed of the extensor carpi radialis brevis, extensor digitorum, extensor digiti minimi, and extensor carpi ulnaris. |
The common extensor group is composed of four muscles: the extensor carpi radialis brevis (ECRB), extensor digitorum, extensor digiti minimi, and extensor carpi ulnaris (Fig. 11.2). The common extensors originate from the lateral epicondyle through the common extensor tendon and are found along the posterolateral aspect of the elbow blending with the more substantial superficial muscle group. The most lateral component of the common extensor tendon is the ECRB, which lies immediately deep to the ECRL. The radiohumeral bursa is an adventitial bursa deep to the ECRB, which may distend in cases of epicondylitis, thereby separating the lateral collateral ligament (LCL) and ECRB (1).
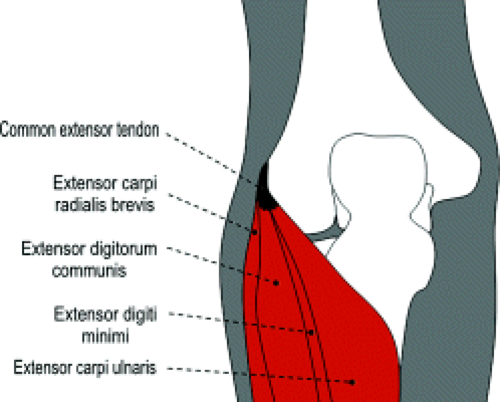 Figure 11.2 Common extensor tendon anatomy. The common extensor group originates from the lateral epicondyle through the common extensor tendon. The extensor carpi radialis brevis also has a significant muscular attachment to the humerus that blends with the more superficial extensor carpi radialis longus. |
The common extensor tendon is seen as a hypointense band arising from the lateral epicondyle on MRI (Fig. 11.3). The ECRB and LCL complex are closely applied to each other and may not be resolved as discrete structures. Some authors suggest that the anatomic origin of the ECRB has contributions from the common extensor tendon, LCL complex, overlying fascia, and intramuscular septum (2, 3). The tendinous origins of the extensor carpi radialis longus and brevis can be distinguished from one another with the ECRL slightly superficial to the ECRB with intervening intermediate signal between the two tendons (Fig. 11.4). The ECRB is the initial site of signal abnormalities in cases of tennis elbow (1). Given the close proximity of the ECRB and lateral ulnar collateral ligament (LUCL), it is not surprising that severe lateral epicondylitis is associated with secondary abnormalities of the LUCL on MRI (4).
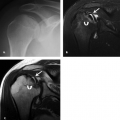
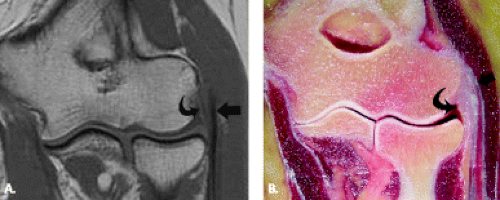 Figure 11.3 Common extensor tendon. A: T1-weighted coronal MR image and B: corresponding specimen photograph show the proximal attachment of the common extensor tendon (straight arrow) arising from the undersurface of the lateral epicondyle. The radial collateral ligament (curved arrow) is closely apposed to its undersurface. |
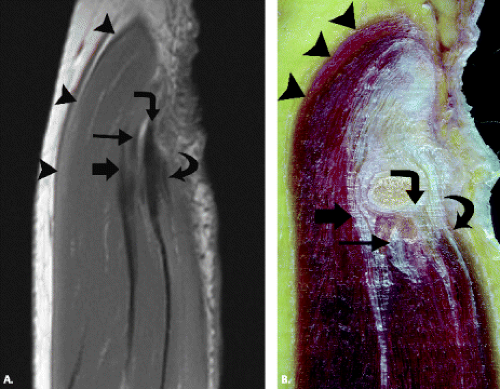 Figure 11.4 Components of the common extensor tendon. A: T1-weighted sagittal MR image and B: corresponding specimen photograph show the relationship of the extensor carpi radialis longus (arrowheads) to the components of the common extensor tendon: extensor carpi radialis brevis (straight arrow), extensor digitorum (thin arrow), extensor digiti minimi (angled arrow), and extensor carpi ulnaris (curved arrow). The narrow low-signal–intensity bands that extend distally to the forearm from the separate muscular contributions represent intermuscular septa that serve as aponeuroses for the individual muscles. |
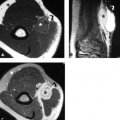
The supinator, the deepest of the lateral muscle group, arises from both the lateral epicondyle and the supinator crest of the ulna, inserting distally on the radial shaft, enveloping much of the proximal radius along its course. The muscle typically has thin superficial and bulky deep components (Fig. 11.5). The posterior interosseous nerve innervates the supinator and travels between the deep and superficial portions of the muscle.
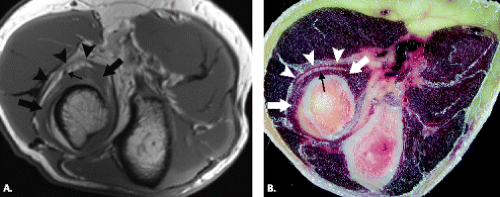 Figure 11.5 Supinator muscle. A: T1-weighted axial MR image and B: corresponding specimen photograph demonstrate its thin superficial (arrowheads) and bulky deep (arrows) components with the interposed posterior interosseous nerve (thin arrow). |
The medial muscle group includes the pronator teres and four superficial flexors: the flexor carpi radialis (FCR), palmaris longus (PL), flexor carpi ulnaris (FCU), and flexor digitorum superficialis (FDS) (Figs. 11.6 and 11.7). The pronator teres forms most of the anteromedial muscle mass at the level of the elbow. The bulk of the pronator teres arises from a large humeral head proximal to the medial epicondyle. A smaller ulnar head of pronator teres arises from the medial aspect of the coronoid process. The pronator teres proceeds distally to insert on the lateral aspect of the radial shaft.
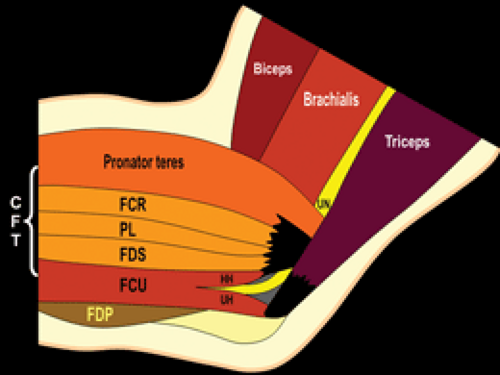 Figure 11.6 Medial muscle and tendon anatomy. The medial muscle group includes the pronator teres and four superficial flexors. |
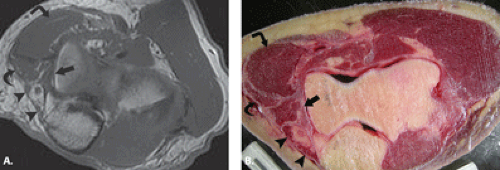 Figure 11.7 Medial muscle anatomy. A: T1-weighted axial MR image and B: corresponding specimen photograph profile components of the medial muscle group: flexor carpi ulnaris (arrowheads), flexor digitorum superficialis (arrow), flexor carpi radialis (curved arrow), and pronator teres (angled arrow). There is no palmaris longus muscle as is noted in 13% of the population. |
The common flexor tendon arises from the medial epicondyle and includes the FCR, PL, FCU, FDS (humeroulnar head), and a portion of the pronator teres (Fig. 11.8). The common flexor muscles at the level of the elbow form a confluent muscular mass at the posteromedial aspect of the joint. On oblique coronal MR images, the common flexor tendon appears as a hypointense band that gradually blends with proximal fibers of the ulnar collateral ligament arising from the undersurface of the medial epicondyle (Fig. 11.9). The palmaris longus, which blends with the posteromedial border of pronator teres, may be absent in up to 13% of cases (5). The FDS arises from two heads, a humeroulnar head arising from the common flexor tendon and a radial head arising from the anterior radius. A fibrous arch is formed where the two heads of the FDS coalesce, beneath which passes the anterior interosseous branch of the median nerve. The FCU also arises from two heads near the cubital tunnel. The first head is the most medial portion of the common flexor tendon and the second head from the medial aspect of the olecranon. A fibrous arch between the two heads forms the roof of the cubital tunnel and has been variously termed the arcuate ligament, Osborne’s band, and the cubital tunnel retinaculum.
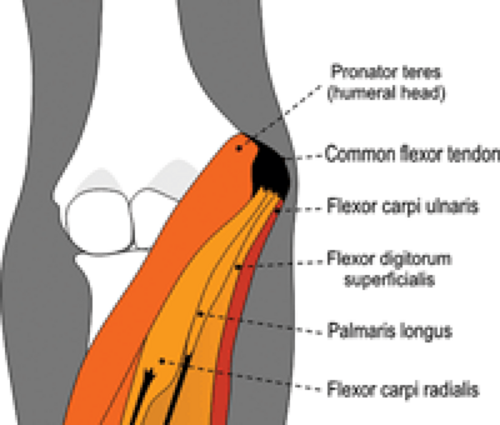 Figure 11.8 Common flexor tendon anatomy. The common flexor tendon arises from the medial epicondyle and includes contributions from the flexor carpi radialis, palmaris longus, flexor carpi ulnaris, humeroulnar head of the flexor digitorum superficialis, and a portion of the pronator teres. |
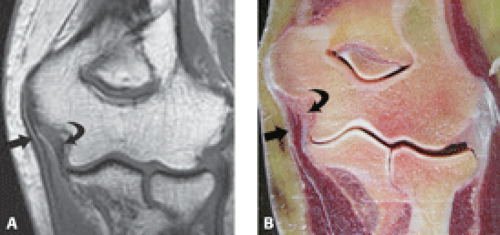 Figure 11.9 Common flexor tendon. A: T1-weighted coronal MR image and B: corresponding specimen photograph show the proximal attachment of the common flexor tendon (straight arrow) arising from the undersurface of the medial epicondyle. The ulnar collateral ligament (curved arrow) is closely apposed to its undersurface. |
The deep flexors include the flexor digitorum profundus and the flexor pollicis longus (FPL). This group originates from the proximal ulna, just distal to the cubital tunnel, thus forming a small muscular mass as the posteromedial aspect of the ulna. Gantzer’s muscle, an accessory slip of the FPL, may be encountered in 45% of individuals and rarely causes impingement of the median nerve (6, 7).
The anterior muscle group includes the two primary flexors of the elbow, the biceps brachii and brachialis. The brachialis arises from the distal humerus and inserts at the ulnar tuberosity. The biceps brachii muscle arises from long and short heads and terminates in a single insertion at the radial tuberosity. The short head arises from the coracoid process and the long head from the supraglenoid tubercle of the scapula. The distal biceps tendon is formed from the two muscle bellies, which unite approximately 7 cm proximal to the elbow. Like the Achilles tendon, the distal biceps tendon has no tendon sheath. The distal portion of the biceps tendon may be at risk for attritional changes and tearing in a fashion similar to the supraspinatus tendon of the shoulder in cases of impingement (8). A relative hypovascular zone has been described in the distal tendon subject to mechanical impingement between the radial tuberosity and ulna (9). The bicipital aponeurosis, or lacertus fibrosis, arises from the distal biceps tendon and passes medially to blend with the fascia covering the flexor–pronator mass of the medial aspect of the elbow (Figs. 11.10 and 11.11). This fibrous band may prevent proximal retraction of the complete biceps rupture, thereby masking the typical clinical findings of a balled-up muscular mass.
 Figure 11.10 Lacertus fibrosis. The lacertus fibrosus, also called the bicipital aponeurosis, arises from the distal biceps tendon and passes medially to blend with the fascial covering of the flexor–pronator group. |
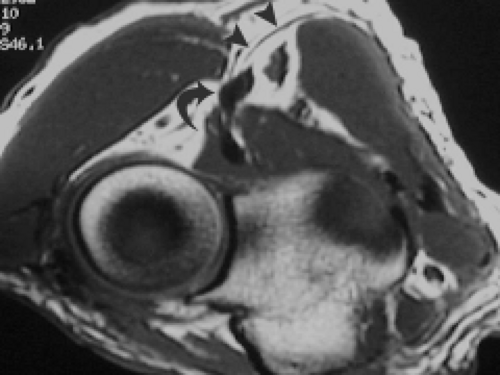 Figure 11.11 Lacertus fibrosis. T1-weighted axial MR image shows the biceps tendon (curved arrow) within the antecubital fossa en route to its ultimate attachment on the radial tuberosity. The lacertus fibrosis (arrowheads) is seen extending from the tendon to the flexor–pronator muscle group. |
Axial images generally provide the best visualization of the biceps tendon as it inserts on the radial tuberosity. Sagittal images of biceps may help confirm suspect pathology. Fluid distension of the bicipitoradial bursa can be easily seen on all three standard imaging planes, although axial images best illustrate the close relation of the bursa and biceps tendon.
The anconeus and triceps form the posterior muscle group. The triceps arises from three heads: the lateral head from the posterolateral proximal humerus, the long head from the infraglenoid tubercle of the scapula, and the medial head from the posterior distal humerus. These form a common tendon that inserts at the olecranon, which normally may have a striated appearance (10). Rarely, a portion of the medial triceps may insert on the medial epicondyle and compress the ulnar nerve (11). The medial head of the triceps may subluxate, causing a snapping sensation similar to that of ulnar nerve subluxation (12). The anconeus arises from the posterior margin of the lateral epicondyle and courses medially to insert on the lateral margin of the olecranon. The role of the anconeus is somewhat controversial, although it is thought to help stabilize the elbow. The triceps insertion is clearly seen on sagittal and axial MR images (Fig. 11.12). The anconeus is easily seen on axial images, serving as a useful landmark for the lateral aspect of the elbow.
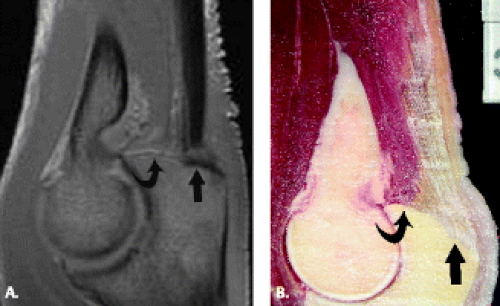 Figure 11.12 Triceps. A: T1-weighted sagittal MR image and B: corresponding specimen photograph shows the combined tendon (arrow) and muscular (curved arrow) attachments of the triceps to the olecranon process. |
The anconeus epitrochlearis is an anomalous muscle found to occur in 11% of anatomic specimens that may cause cubital tunnel syndrome (13). In addition, there have been reports of symptomatic muscle edema in this accessory muscle as an additional cause of medial elbow pain (14). The anconeus epitrochlearis arises from the medial humeral condyle, passes superficial to the ulnar nerve, and inserts on the olecranon (Fig. 11.13).
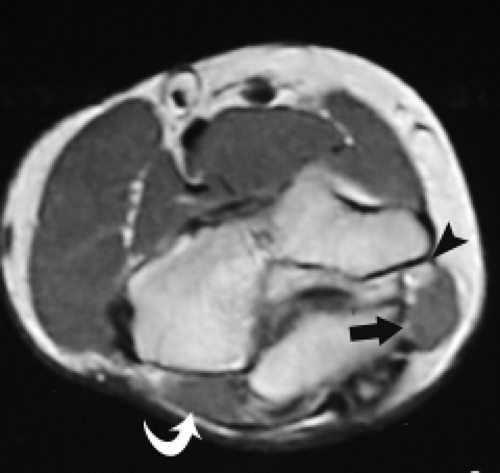 Figure 11.13 Anconeus epitrochlearis. T1-weighted axial MR image demonstrates an accessory muscle, the anconeus epitrochlearis (arrow), posterior to the medial epicondyle and ulnar nerve (arrowhead). The anconeus (curved arrow) muscle is noted at the radial side of the joint. The close approximation and mass effect of the muscle on the subjacent nerve explain the association of this condition with ulnar neuritis and the cubital tunnel syndrome. |
Tendon Lesion Classification and Imaging Characterization
Like elsewhere in the body, the tendons about the elbow should be smooth, linear structures of low signal intensity. The distinction between tendinosis and tendon tear with MRI can be challenging. Abnormal morphology (attenuation or thickening) can be seen in tendinosis or tear. It is the presence of increased signal intensity within the substance of a tendon, that which parallels simple fluid on a fluid-sensitive or long TE sequence, that heralds the presence of a tear and allows the distinction between tendinosis and tendon tear. Increased signal intensity within a tendon that does not brighten to the level of fluid on fluid-sensitive sequences, rather, is classified as tendinosis (Fig. 11.14). With regard to the short TE sequences, increased signal intensity can be identified in both tendinosis and tear. An alternative explanation for increased intratendon signal intensity with short echo times is the “magic angle” phenomenon encountered when tendons are placed at an angle of 45 to 65 degrees to the static magnetic field. In the fully extended elbow, however, the angle of the tendons just beyond their origins from the humeral epicondyles is much less than 45 degrees, lessening the effect of this phenomenon significantly (15).
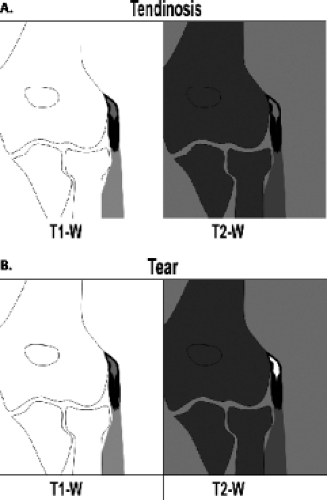 Figure 11.14 Signal intensity changes in tendinosis versus tendon tear. A: In the setting of tendinosis, signal changes encountered on T1-weighted images should not brighten to the level of simple fluid on long TE sequences (proton density- or T2-weighted), B: whereas with tendon tears, these changes brighten to the level of fluid on long TE sequences. |
Pathologic lesions within tendons should be carefully characterized with regard to degree of abnormality as well as localization. Like in the shoulder tendons, elbow tendon tears are described as partial or complete. A complete tear is diagnosed by a focal area of discontinuity (Fig. 11.15). Partial tears are further described by their location within the tendon. They are described as articular side, intrasubstance, or superficial in nature (Fig. 11.16). It is the preference of the author to further characterize the degree of tendon tear as low grade (less than 50% of the width of the tendon), moderate grade (50% of the width of the tendon), or high grade (greater than 50% of the width of the tendon). This system uses the internal standard of the patient’s own tendon width to help approximate the degree of abnormality identified by imaging. In addition, all lesions should be localized with regard to location within the tendon, from attachment site to musculotendinous junction.
 Figure 11.15 Full-thickness tendon tears. Full-thickness tears of the tendon are characterized by complete discontinuity of tendon fibers. |
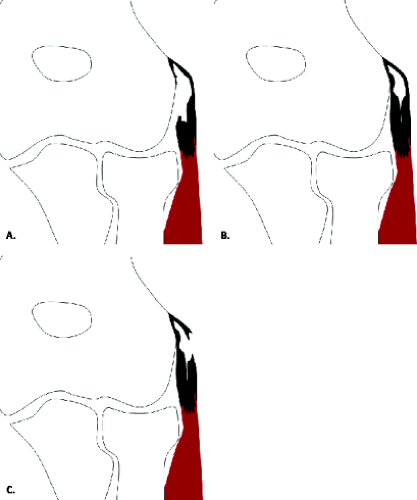 Figure 11.16 Characterization of partial-thickness tendon tears. Partial-thickness tears of the tendon are characterized as A: articular-, B: intrasubstance-, or C: superficial-sided. |
Epicondylitis and Overuse Syndromes
The clinical entity of epicondylitis is the most common source of elbow pain in the general population with lateral epicondylitis occurring seven to 20 times more frequently than its medial counterpart with an incidence of
four to seven per 1000 patients seen in general practice (16–18). Although the term “epicondylitis” suggests an inflammatory process, the current consensus based on clinical and surgical evidence suggests that the underlying pathology within the tendon is that of microtears resulting in mucoid degeneration and neovascularization (1, 19, 20). Nirschl and Pettrone (3) described a characteristic microscopic appearance of “angiofibroblastic hyperplasia” of the involved tissue. The normal parallel orientation of collagen fibers is disrupted by an invasion of fibroblasts and vascular granulation-like tissue without an acute or chronic inflammatory component. In the series of surgically treated elbows reported by Nirschl and Pettrone, 97% (n = 88) demonstrated varying amounts of this gross pathologic tissue at the origin of the extensor carpi radialis brevis tendon; 35% also demonstrated gross tendon rupture. In addition to the chronic fibrous and vascular granulation tissue noted by Nirschl and Pettrone, Goldie (21) revealed the presence of free nerve endings within the tissue at the site of lateral epicondylitis, possibly explaining the symptomatic nature of this process. For the purposes of imaging diagnosis, it is the preference of the author to characterize the imaging appearance of the tendon as normal, tendinotic, or torn. Either the presence of tear or tendinosis could be consistent with the clinical entity of epicondylitis.
four to seven per 1000 patients seen in general practice (16–18). Although the term “epicondylitis” suggests an inflammatory process, the current consensus based on clinical and surgical evidence suggests that the underlying pathology within the tendon is that of microtears resulting in mucoid degeneration and neovascularization (1, 19, 20). Nirschl and Pettrone (3) described a characteristic microscopic appearance of “angiofibroblastic hyperplasia” of the involved tissue. The normal parallel orientation of collagen fibers is disrupted by an invasion of fibroblasts and vascular granulation-like tissue without an acute or chronic inflammatory component. In the series of surgically treated elbows reported by Nirschl and Pettrone, 97% (n = 88) demonstrated varying amounts of this gross pathologic tissue at the origin of the extensor carpi radialis brevis tendon; 35% also demonstrated gross tendon rupture. In addition to the chronic fibrous and vascular granulation tissue noted by Nirschl and Pettrone, Goldie (21) revealed the presence of free nerve endings within the tissue at the site of lateral epicondylitis, possibly explaining the symptomatic nature of this process. For the purposes of imaging diagnosis, it is the preference of the author to characterize the imaging appearance of the tendon as normal, tendinotic, or torn. Either the presence of tear or tendinosis could be consistent with the clinical entity of epicondylitis.
Lateral Epicondylitis
Clinical Diagnosis.
As previously mentioned, lateral epicondylitis is a common source of elbow pain, first described over 100 years ago in a tennis player. This entity represents a pathologic condition of the common extensor muscles at their origin on the lateral epicondyle and is characterized by pain in that area on physical examination. The area of maximal tenderness lies 2 to 5 mm distal and anterior to the midpoint of the lateral epicondyle (19). Resisted wrist and finger extension with the elbow in full extension can intensify pain, whereas range of motion and sensation are generally normal. In some cases, wrist extensor weakness secondary to pain may be detected by the astute clinician. The clinical diagnosis is generally straightforward but can be confused with other causes for lateral-sided elbow pain. These causes include many of the previous theories posed to explain the pathophysiology of lateral epicondylitis: inflammation of an extra-articular radial humeral bursa, inflamed synovial fringe, fibrosis of the annular ligament, radial or posterior interosseous nerve entrapment, radiocapitellar chondromalacia, and cervical radiculopathy
(19, 22–25). Clearly, MRI with its excellent soft tissue contrast and multiplanar imaging capabilities can be helpful in distinguishing between the aforementioned sources of lateral elbow pain.
(19, 22–25). Clearly, MRI with its excellent soft tissue contrast and multiplanar imaging capabilities can be helpful in distinguishing between the aforementioned sources of lateral elbow pain.
Mechanism.
As previously noted, current theories indicate that lateral epicondylitis appears to begin as a microtear, usually in the origin of the extensor carpi radialis brevis, with formation of subsequent fibrosis and granulation tissue as a consequence of chronic repetitive microtrauma (3, 26). Activities that require forceful and repetitive forearm dorsiflexion, radial deviation, and supination stress the wrist extensors. Occupational activities that lead to epicondylitis include meat cutting, plumbing, painting, raking, and weaving. Recreational activities implicated in lateral epicondylitis include racquet sports such as squash, racquetball, and tennis, hence the moniker “tennis elbow.” This biomechanical overload has been demonstrated by electromyographic (EMG) studies that analyzed the activity of the muscles that stabilize the elbow while playing tennis. These studies showed the greatest activity during ground strokes to be within the musculotendinous unit stabilizing the wrist, in decreasing order: the ECRB followed by the ECRL and the extensor digitorum communis. These data support the theory that the ECRB, by overuse, is the musculotendinous unit most prone to be affected in this condition (27).
Further exploration into the specific components of overuse that result in the clinical expression of lateral epicondylitis suggest that increased age of the patient as well as increased time performing the offending activity play a role in the development of symptoms (19). Studies analyzing the two-handed versus single-handed backhand in tennis investigated the theory that players using the double-handed backhand rarely developed lateral epicondylitis because the helping hand both absorbs energy lessening the stress on the dominant hand as well as changes the mechanics of the swing. Giangarra et al. (28) found that extensor EMG activity was not decreased in the case of the double- versus single-handed backhand. Moreover, it was discovered that the activity in the helping and dominant hands was not significantly different from each other or from the single-handed technique. These results suggest that technique may be one of the most important factors in the development of symptomatic structural changes in the setting of overuse of the common extensor tendon and its components.
Imaging Diagnosis.
As previously noted, the MRI diagnosis of pathology in the common extensor tendon focuses primarily on signal intensity and morphology changes to distinguish between tendinosis and tear. The common extensor tendon is best visualized in the oblique coronal imaging plane, arising from the undersurface of the lateral epicondyle, closely apposed to portions of the radial collateral ligament complex. It is imperative that a sequence with optimal fluid sensitivity and signal-to-noise resolution is included in the imaging protocol of the elbow. In a meta-analysis of the MR findings of humeral epicondylitis, four of seven studies included in the analysis used either a T2-weighted fat-suppressed imaging sequence or an inversion recovery sequence in the imaging protocol (17). As noted in the “Technical Considerations” chapter, some authors do use gradient recalled echo imaging sequences for evaluation of tendons and ligaments about the elbow (1). It is the bias of the authors to use fat suppression in conjunction with T2-weighted fast spin-echo imaging to improve conspicuity of signal changes in an effort to facilitate the distinction of tendinosis versus tears of tendons.
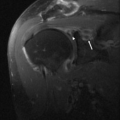
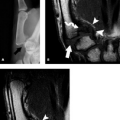
The MRI diagnosis of the clinical entity of lateral epicondylitis includes abnormal morphology and signal intensity of the common extensor tendon. Several imaging findings have been associated with the clinical entity of lateral epicondylitis. Not all studies localize tendon abnormalities to the specific components of the common extensor tendon; however, those that do attempt to localize it show pathology primarily in the ECRB (1, 15, 29–32). The spectrum of pathology encountered on MRI studies in this clinical entity includes abnormal separation of the radial collateral ligament and the ECRB with granulation tissue (Fig. 11.17). Potter et al. (1) showed this finding in 10 of 20 patients with lateral epicondylitis Savnik et al. (32) in 25 of 30 patients. In a recent study of 11 patients with the clinical diagnosis of refractory lateral epicondylitis, MRI demonstrated findings that suggested granulation tissue within the ECRB (n = 6). Enucleation of the granulation tissue provided symptomatic relief in all six symptomatic patients, underlining
the importance of MRI as a decision-making tool in the treatment of this entity (33). The vast majority of patients with lateral epicondylitis show abnormal morphology of the ECRB in the form of abnormal thickening with abnormal signal intensity on the short TE sequences establishing the underlying diagnosis of tendinosis (Fig. 11.18). It must be emphasized that the imaging findings of tendinosis must be correlated with the clinical presentation before the diagnosis of lateral epicondylitis is made. In many studies, asymptomatic volunteers comprising a control group were discovered to have abnormal morphology and signal intensity of the tendon (1, 15, 32). In the absence of clinical symptoms, imaging findings likely represent subclinical tendinosis or early tendon degeneration.
the importance of MRI as a decision-making tool in the treatment of this entity (33). The vast majority of patients with lateral epicondylitis show abnormal morphology of the ECRB in the form of abnormal thickening with abnormal signal intensity on the short TE sequences establishing the underlying diagnosis of tendinosis (Fig. 11.18). It must be emphasized that the imaging findings of tendinosis must be correlated with the clinical presentation before the diagnosis of lateral epicondylitis is made. In many studies, asymptomatic volunteers comprising a control group were discovered to have abnormal morphology and signal intensity of the tendon (1, 15, 32). In the absence of clinical symptoms, imaging findings likely represent subclinical tendinosis or early tendon degeneration.
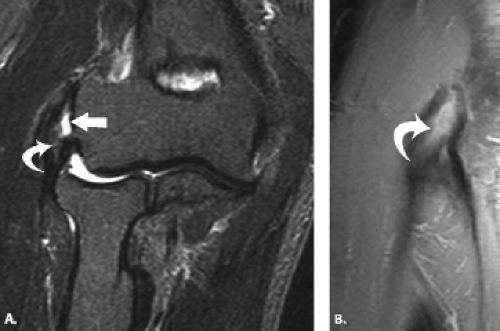 Figure 11.17 Common extensor tendon pathology and granulation tissue. A: T2-weighted fat-suppressed coronal MR image through the elbow shows a partial articular-sided tear (arrow) manifested by high signal intensity within the common extensor tendon. Intermediate signal intensity material representing granulation tissue (curved arrow) is present between the radial collateral ligament and the common extensor tendon. B: Proton density-weighted fat-suppressed sagittal MR image through the common extensor tendon shows the intermediate-signal–intensity granulation tissue (curved arrow). |
 Figure 11.18 Common extensor tendinosis. A: T1-weighted and B:
Get Clinical Tree app for offline access
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|