Osteoporosis is a generalized metabolic bone disease characterized by insufficient formation or increased resorption of bone matrix that results in decreased bone mass and microarchitectural deterioration of bone. Although there is a reduction in the amount of bone tissue, the tissue present is still fully mineralized. In other words, the bone is quantitatively deficient but qualitatively normal.
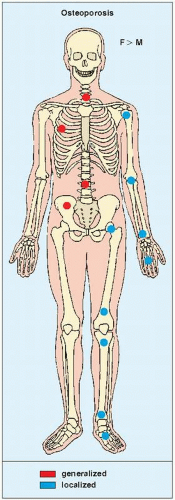
Osteoporosis has a variety of possible causes and consequently manifests in a number of different forms (Table 27.1). The basic distinction in osteoporosis is between those types that are generalized or diffuse, involving the entire skeleton, and those that are localized to a single region or bone (regional) (Fig. 27.1). The basic distinction between possible causes is between those that are congenital and those that are acquired.
Generalized Osteoporosis
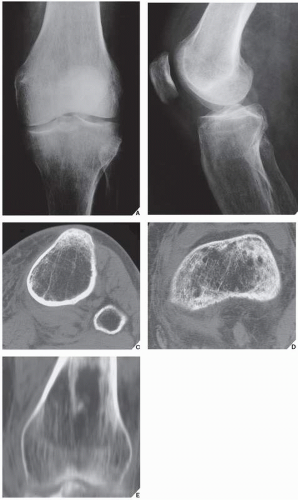
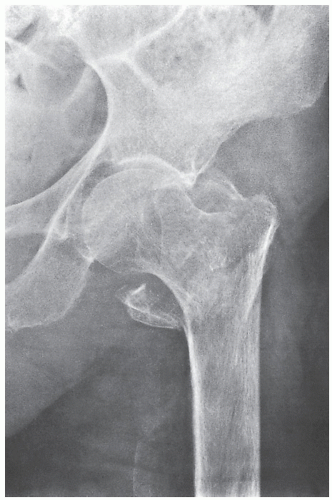
Certain radiographic features are common to virtually all forms of osteoporosis, regardless of their specific cause. There are always some diminution of cortical thickness and decrease in the number and thickness of the spongy bone trabeculae (Fig. 27.2). These changes are more prominent in non-weight-bearing segments and those not subject to stress. The first sites affected by osteoporosis, as well as the ones that are best demonstrated on radiographic study, are the periarticular regions, where the cortex is anatomically thinner (Fig. 27.3). In the long bones, the thickness of the cortices decreases, the bones become brittle, and there is increased clinical incidence of fractures, particularly of the proximal femur (Fig. 27.4), the proximal humerus, the distal radius, and the ribs.
Besides quantitative computed tomography (QCT) and other methods of evaluating osteoporosis (discussed in detail in Chapter 26), some simple methods using conventional radiography have been developed.
The analysis of the trabecular pattern of the bones has been emphasized as an effective method to evaluate osteoporosis, since patterns of trabecular loss correlate well with increasing severity of osteoporosis.
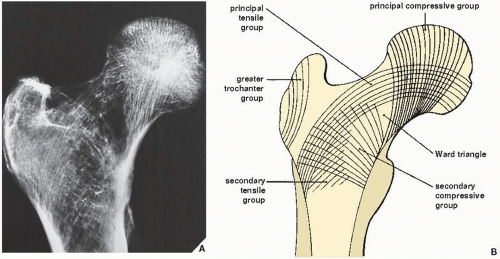
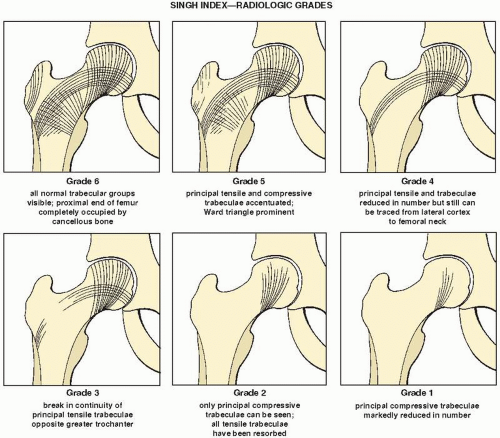
In the femur, these changes may be evaluated using the Singh index, which is based on the trabecular architecture of the proximal femur— namely, the pattern of the principal compressive group of trabeculae, the secondary compressive group of trabeculae, and the principal tensile group of trabeculae (Fig. 27.5 and Table 27.2). The trabecular pattern of the proximal end of the femur is an excellent indicator of the severity of the osteoporosis. Singh has shown that trabecular loss occurs in a predictable sequence that can be used to grade the severity of osteopenia. He recognized that the compressive trabeculae were more essential than the tensile trabeculae, and that the peripherally located trabeculae were more vital than central ones.
Six radiologic grades have been defined according to the trabecular pattern (Fig. 27.6).
In early osteoporosis, both the compressive and tensile trabeculae are accentuated because of initial resorption of the randomly oriented trabeculae, and thus the radiolucency of the Ward triangle becomes more prominent. With increasing severity of osteoporosis, the tensile trabeculae are reduced in number and regress from the medial femoral border to the lateral. When trabecular resorption increases, the outer portion of the principal tensile trabeculae opposite the greater trochanter disappear, opening the Ward triangle laterally. As osteoporosis increases in severity, resorption of all trabeculae occurs, with the exception of those in the principal compressive group. In advanced osteoporosis, the principal compressive component is the last to be involved, a process manifested by a decrease in the number and length of individual trabeculae. Eventually, the upper femur may be completely devoid of all trabecular markings.
The other major area in which osteoporotic changes are evaluated is the axial skeleton, particularly the spine. This is especially true in osteoporosis associated with aging, that is, involutional (senescent and postmenopausal) osteoporosis, in which the vertebral bodies are particularly vulnerable. Initially, there is a relative increase in the density of the vertebral end plates due to resorption of the spongy bone, causing what is called an “empty box” appearance (Fig. 27.7). Later, there is an overall decrease in density with a loss of any trabecular pattern, creating a “ground glass” appearance. A typical feature of vertebral involvement in osteoporosis is biconcavity of the body, which exhibits a “fish mouth” appearance (“codfish vertebrae”) (Fig. 27.8). This presentation results from expansion of the disks, leading to arch-like indentations on both superior and inferior margins of the weakened vertebral bodies. In advanced stages, there is complete collapse of the vertebral body associated with a wedge-shaped deformity. In the thoracic spine, this leads to increased kyphosis.
Of special interest in generalized osteoporosis are the three major varieties of iatrogenic osteoporosis. Heparin-induced osteoporosis may develop after long-term, high-dose daily heparin treatment (more than 10,000 units). Precisely how this type of osteoporosis is initiated and develops is not clearly understood, although osteoclastic stimulation and osteoblastic inhibition with suppressed endochondral ossification have been implicated as potential causes. Spontaneous fractures of the vertebrae, ribs, and femoral neck are noted on radiographic studies. Dilantin-induced osteoporosis occasionally develops after prolonged use of phenytoin (Dilantin). The vertebral column and ribs are usually affected, and fractures are a common complication.
Transient osteoporosis of the hip Regional migratory osteoporosis Idiopathic juvenile osteoporosis
Paget disease (hot phase)
Endocrine
Steroid induced
Hyperthyroidism
Miscellaneous
Hyperparathyroidism Cushing syndrome
Involutional (senescent/postmenopausal)
Acromegaly
Amyloidosis
Estrogen deficiency
Ochronosis
Hypogonadism
Paraplegia
Diabetes mellitus
Weightlessness
Pregnancy
Idiopathic
FIGURE 27.1 Target sites of osteoporosis.
FIGURE 27.2 Generalized osteoporosis. Anteroposterior (A) and lateral (B) radiographs of the left knee of an 82-year-old man reveal increased radiolucency of bones, thinning of the cortices, and sparse trabecular pattern. These changes are more effectively demonstrated on axial CT sections obtained through the proximal tibia (C) and distal femur (D), as well as on reformatted coronal image of the distal femur (E).
FIGURE 27.3 Periarticular osteoporosis. Anteroposterior (A) and lateral (B) radiographs of an ankle reveal sparse trabecular pattern and increase radiolucency in the subchondral areas.
FIGURE 27.4 Osteoporosis complicated by a fracture. An 85-year-old woman with advanced postmenopausal osteoporosis sustained an intertrochanteric fracture of the left femur, as seen on this anteroposterior radiograph. Note the thinning of the cortex and the increased radiolucency of the bones.
FIGURE 27.5 The Singh trabecular index. (A) The trabecular pattern of the proximal end of the femur is an excellent indicator of the severity of the osteoporosis. (B) The trabecular arcades are important to the Singh trabecular index. Confluence of principal tensile, principal compressive, and secondary compressive trabeculae in the femoral neck forms a triangular region of radiolucency, the Ward triangle. The principal tensile trabeculae are more important than the secondary trabeculae; the compressive trabeculae are more important than the tensile trabeculae. Bone loss occurs in order of increasing importance. (Modified from Singh M et al., 1970, with permission.)
TABLE 27.2 The Five Major Groups of Trabeculae
Principal Compressive Group
Extend from medial cortex of femoral neck to superior part of femoral head
Major weight-bearing trabeculae
In normal femur are the thickest and most densely packed
Appear accentuated in osteoporosis
Last to be obliterated
Secondary Compressive Group
Originate at the cortex, near the lesser trochanter
Curve upward and laterally toward the greater trochanter and upper femoral neck
Characteristically thin and widely separated
Principal Tensile Group
Originate from the lateral cortex, inferior to the greater trochanter
Extend in an arch-like configuration medially, terminating in the inferior portion of the femoral head
Secondary Tensile Group
Arise from the lateral cortex below the principal tensile group
Extend superiorly and medially to terminate after crossing the middle of the femoral neck
Greater Trochanter Group
Composed of slender and poorly defined tensile trabeculae
Arise laterally below the greater trochanter
Extend upward to terminate near the greater trochanter’s superior surface
FIGURE 27.6 Singh index—radiologic grades. (Modified from Singh M et al., 1970, with permission.)
Steroid-induced osteoporosis, occurring either during the course of Cushing syndrome or iatrogenically during treatment with various corticosteroids, is characterized by decreased bone formation and increased bone resorption. Although the axial skeleton is most often affected, the appendicular skeleton may also be involved. In the spine, considerable thickening and sclerosis of the vertebral end plates occur without a concomitant change in the anterior and posterior vertebral margins.
Osteoporosis associated with neoplastic processes is discussed in Chapter 16.
Only gold members can continue reading. Log In or Register to continue

 Miscellaneous Metabolic and Endocrine Disorders
Miscellaneous Metabolic and Endocrine Disorders
 Benign Tumors and Tumor-like Lesions III: Fibrous, Fibroosseus, and Fibrohistiocytic Lesions
Benign Tumors and Tumor-like Lesions III: Fibrous, Fibroosseus, and Fibrohistiocytic Lesions
 Upper Limb III: Distal Forearm, Wrist, and Hand
Upper Limb III: Distal Forearm, Wrist, and Hand
 Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
 Upper Limb III: Distal Forearm, Wrist, and Hand
Upper Limb III: Distal Forearm, Wrist, and Hand



