FIG. 9.1 ● Dose calibrator. It is a gas-filled ionization chamber used to measure radioactivity. The sample to be measured is placed in the shielded ionization chamber.
Accuracy
Accuracy should be checked at installation, annually, and after repair or when the instrument is moved to a new location within the clinic. Accuracy is a measure of the readings of the dose calibrator in comparison with the well-accepted standards. Long-lived radionuclides such as 57Co (half-life 270 days) and 137Cs (half-life 30 years) are measured repeatedly in the dose calibrator, and average readings are compared with the values issued by National institute of Standards and Technology (NIST). If the reading differs by more than 10% of standards, the instrument should not be used.1
Constancy
Constancy should be checked daily. For the constancy test, a reference source such as (57Co, 133Ba, 68Ge, or 137Cs) is placed in the dose calibrator, and the activity reading on each scale is recorded; day-to-day readings should agree within 10%. The readings at each predefined setting for different radionuclides used in the nuclear medicine department (99mTc, 131I, 123I, 111In, etc.) are recorded and compared with previous readings.
Linearity should be checked at the installation of the device, quarterly, when the instrument is moved from one place to another, and after repairs. For the quarterly check of linearity by the decay method, a high activity (~37 GBq) of Tc-99m is independently calibrated and then the measurements are repeated at 12-hour intervals over three consecutive days. Over that time, which is equivalent to 12 half-lives of 99mTc, the activity decays to about 11 MBq. The measured activities are then plotted versus time on a semilogarithmic graph, and the best-fit straight line drawn through the data points is plotted. For each data point, the difference between the measured activity and the activity on the best-fit straight line at that point should be less than 10%. To save time, a more rapid technique known as the shield method is used. In this technique, lead sleeves of increasing thickness are placed in the dose calibrator with a 99mTc source (Fig. 9.2). The thickness of sleeves is such that when used both individually and in combination they effectively reproduce the decline in the activity of Tc-99m over 96 hours.
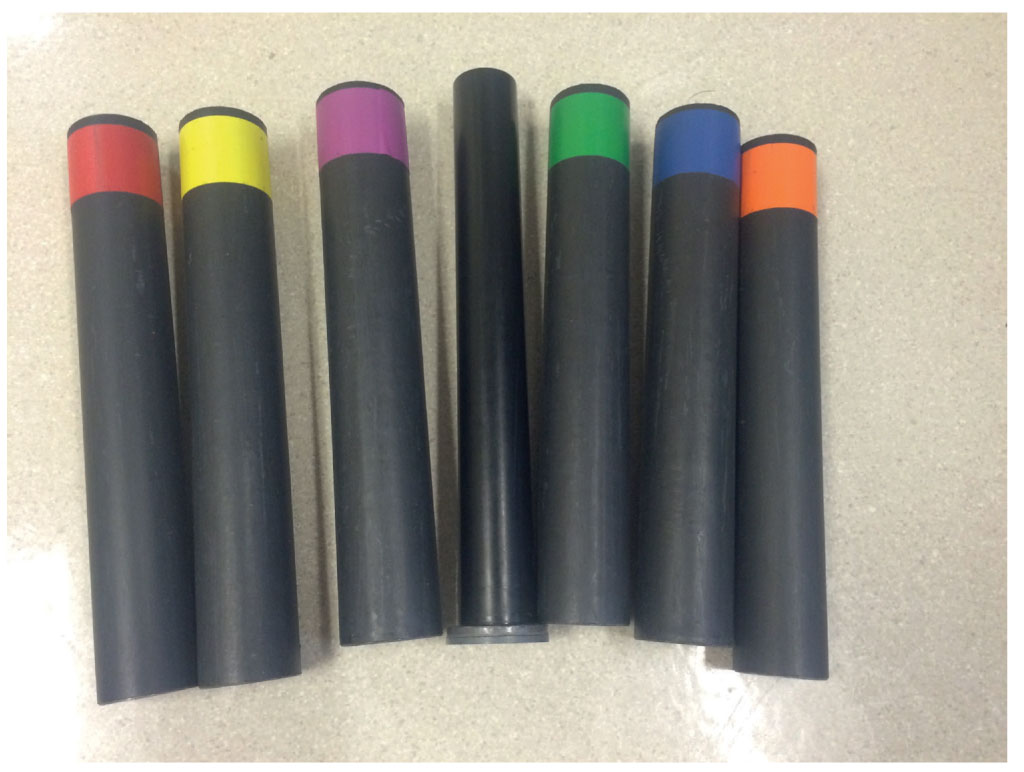
FIG. 9.2 ● Lead sleeves. A set of lead-lined plastic sleeves for evaluation of dose-calibrator linearity by shield method.
Geometry
The effect of sample geometry should be checked at installation and after repairs. The apparent activity of a dose will vary with the volume and shape of the container, as well as the position of the dose placed within the chamber of a dose calibrator. Dose measurements should not vary by more than 10% when the sample is measured in different types of containers such as vials, syringes, or bottles. The sample geometry can also be checked by placing a small amount of activity at the bottom of the container and then progressively adding a diluent such as water.
Survey Meters
Survey meters are an important component of any nuclear medicine department. They are portable, battery-operated, gas-filled ionization chambers or solid-state scintillation detectors used to measure exposure rates (e.g., in mR/h) or counting rates (e.g., in counts per minute [CPM]). The most familiar ones are Geiger counter and pocket dosimeters. Geiger counters are of high sensitivity and are well suited for low-level surveys, for example, for checking radioactive contamination (Fig. 9.3A, B). Cutie-pies are another type of survey meter that have relatively low-sensitivity ionization chambers and are designed for use where high fluxes of X- and γ-rays are encountered. Generally, cutie-pies are calibrated in exposure rates (mR/h) and Geiger counters in counting rates (cpm). QC of survey meters include a battery check, background check, constancy, and calibration.1,2
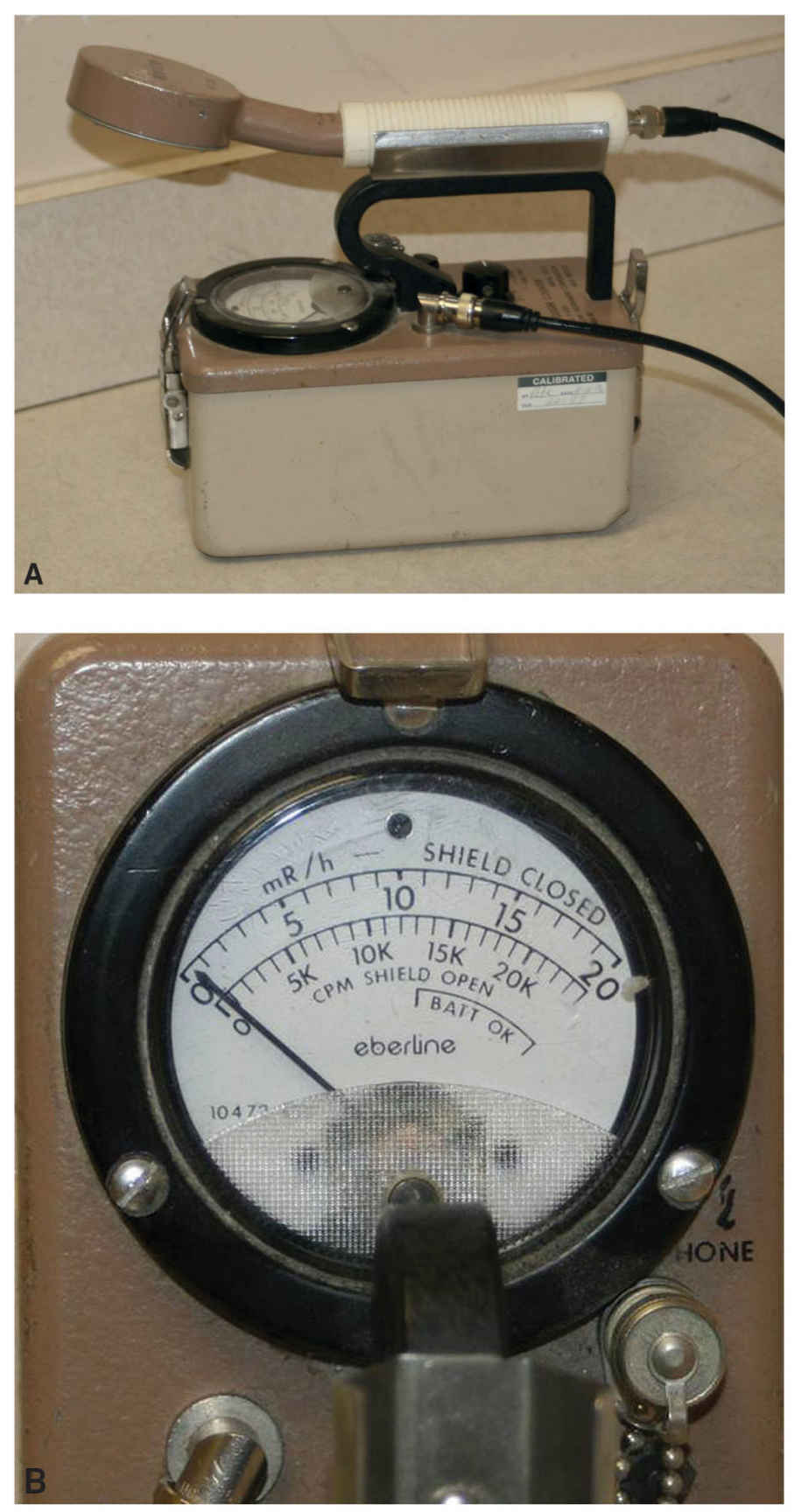
FIG. 9.3 ● Geiger–Mueller survey meter. A: This is used to measure low levels of radiation. A pancake detector is located at the end of the detector. A calibration sticker is attached. B: The dial reads in either counts per minute (CPM) or milliroentgens per hour (mR/hr).
Battery Check
The battery should be checked daily, with a display indicating whether the voltage supplied by the battery is within the acceptable operating range.
Background Check
Background check should be performed daily to ensure that the survey meter has not been contaminated, and the background exposure or counting rate is performed daily in an area well away from the radioactive sources within the department.
A long-live radionuclide should be checked daily to ensure that the survey meter reading of the source remains constant, that is, within 10% of its original value. The survey meter should be recalibrated if the reading differs by more than 10% of original value.
Calibration
Calibration should be performed at installation, after repairs, and annually. All survey meters should be checked for accuracy using long-lived radionuclides. The readings are taken from two long-lived radionuclide sources at incremental distances from the sources (such as every 10th of a meter up to 1 m). The readings must be within 20% of their expected measurement. Many nuclear medicine facilities have their survey meters calibrated by the institutional radiation safety office or by a commercial calibration laboratory. The measurement procedure, the measured and expected exposure rates, and a dated sticker summarizing the calibration results are affixed to the meter itself.
Scintillation Detectors
Scintillation detectors include well counters and organ uptake probes. Well counters are of high sensitivity and are used for counting of radioactive specimens such as blood or urine samples or wipe tests for survey of removable contamination (Fig. 9.4). Counting results are expressed in activity (e.g., μCi), using the appropriate isotope-specific calibration factor (μCi/cpm). Routine QC includes energy peaking and background check, constancy, energy resolution, calibration, and efficiency.3
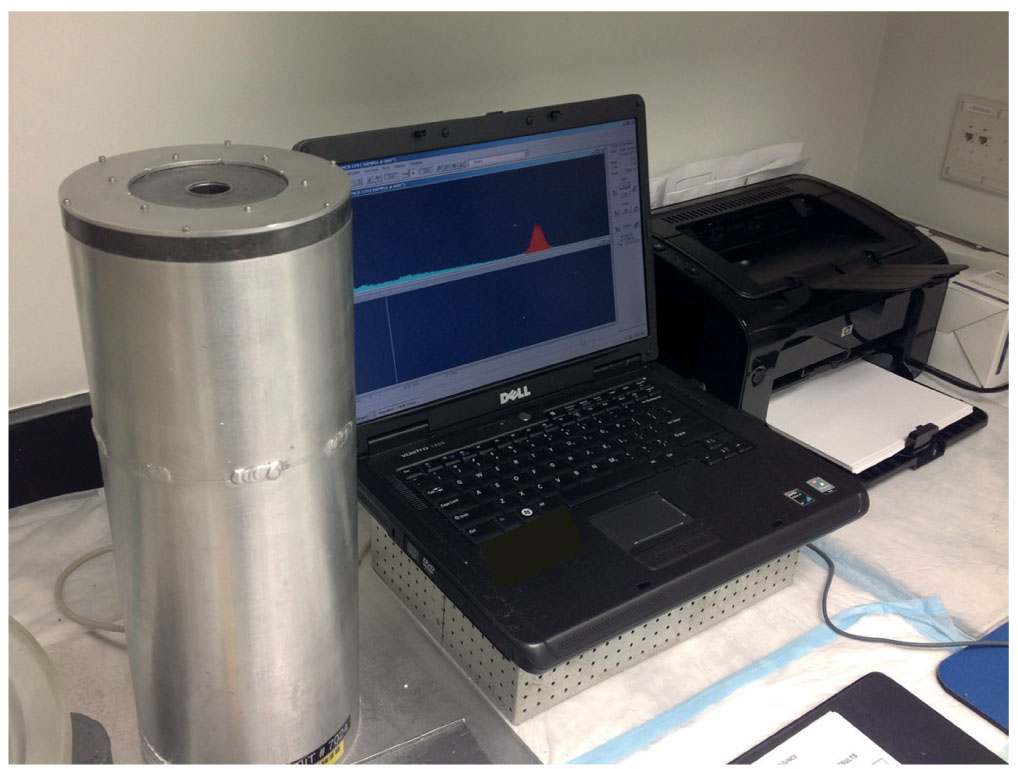
FIG. 9.4 ● Well counter. Well counters are high-sensitivity heavily shielded scintillation crystals used for counting of radioactive specimens such as blood or urine samples or wipe tests for survey of removable contamination.
Energy Peaking and Background Check
Routine checks of the photopeak energy window (i.e., energy peaking) are performed if the counter is equipped with a multichannel analyzer (MCA) and a background check. Before counting samples containing a particular radionuclide, the energy spectrum is checked to verify that the counter is properly peaked so that the photopeak of the radionuclide coincides with the preset photopeak energy window. Isotope-specific radionuclide counting or imaging with a scintillation detector is commonly done using a 20% photopeak energy window, equivalent to an energy range of Eγ ± 10% (i.e., 0.9 to 1.1 Eγ), where Eγ is the X- or γ-ray energy of the radionuclide. This is performed daily.
Energy Resolution
Energy resolution (percentage full width at half-maximum) should be checked at least quarterly using a reference-source radionuclide such as 57Co. Energy resolution is the ability of a counter to discriminate between light pulses caused by gamma rays of different energies. The full width half-maximum (FWHM) of the photopeak should be less than 10% of the energy of the photopeak.
Calibration
Calibration is performed on a daily basis using a long-lived radionuclide source (such as 137Cs), which is placed in the well counter or in front of the probe.
Efficiency
Efficiency check is performed annually. Efficiency check is performed using reference standard sources with emission sources with similar energy emissions to the radionuclides measured routinely in the counter or in front of the thyroid/organ probe. The efficiency of the thyroid probe or well counter can be calculated using the following equation:
Efficiency= [(counts per minute of standard) – (counts per minute of background)] × [(activity of standard in microcurie)]–1.

FIG. 9.5 ● Organ uptake probe system. This includes a single crystal, thyroid/organ probe for measuring radionuclide uptake.
Intraoperative Probes
Intraoperative probes are solid or semisolid state detectors. They are highly collimated handheld devices that are commonly used in surgical practice for sentinel node localization in different types of cancer (e.g., breast cancer, melanoma, etc.). The different QC tests include daily battery check, bias check, and background check. A daily bias check should be performed for both the primary and any back-up battery to verify that bias voltage is within acceptable limits. Other tests include daily counting rate constancy using long-lived reference sources such as 157Co and 133Ba. A change of ±10% in the net counting rate from one day to the next indicates an inappropriate window setting.3
Organ Uptake Probes
Organ uptake probes have been commonly used to measure thyroid uptake and are commonly known as thyroid uptake probes (Fig. 9.5
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


