Shazia Ashfaq, MD
INTRODUCTION
A sign is a mark carrying a conventional meaning and used in place of words to convey a complex notion. In medicine, a sign is an objective evidence of disease specially observed and interpreted by a physician. Multiple signs are described in the radiology literature. The recognition of these signs allows the radiologist and the clinician to make a specific diagnosis or give a brief differential diagnosis. We have compiled a collage of easily recognizable signs in musculoskeletal radiology. Familiarity with these signs can direct the radiologist toward an accurate diagnosis, timely intervention, and astute management. These signs are illustrated with radiographs to help elucidate direct or indirect evidence of the pathology and mechanism of injury. Findings are best appreciated on different imaging modalities; for example, an axial computed tomography (CT) image of the spine will confirm spondylolisthesis suspected on a radiograph.
The adage, a picture is worth a thousand words, is true in this context. However, pattern recognition requires practice. Familiarization with these signs helps build a mental archive for image recall.
ABSENT BOW TIE SIGN1
Introduction and Anatomical Context: Normal menisci can be seen as a series of hypointense classic bow ties on sagittal magnetic resonance imaging (MRI). The knee joint is cushioned by fibrocartilaginous medial and lateral menisci. The menisci lie along the margin of proximal tibial articular surface. Menisci act as shock absorbers and allow smooth movement of joint surfaces over each other.
Etiology: Post-traumatic. Medial meniscus is more commonly injured than lateral meniscus. Most common cause of lateral meniscus injury is a discoid meniscus (Figure 11-1).
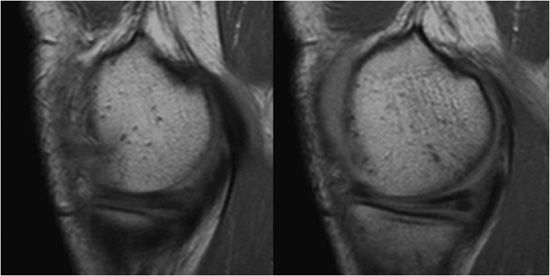
Figure 11-1. Absent bow tie. Two consecutive sagittal cuts of proton density MRIs of the peripheral medial meniscus of the knee.
Radiological Findings: The second image reveals loss of the normal bow tie appearance of the meniscus. The “absent bow tie” is a good sign of a bucket handle tear of the meniscus. The absence of the normal bow tie is secondary to the displaced fragment that makes up the “handle” of the bucket. The absent bow tie sign mandates that at least two adjacent sagittal images with a normal meniscal body segment appearance are not present. A word of caution is dependent on the cuts; sometimes one of the two bow ties may be absent without a real bucket handle tear. Therefore, correlation with the coronal and axial images can be helpful.
Diagnosis: Bucket handle tear of menisci.
Imaging Modality: MRI.
PEARLS
![]() Absent bow tie sign is present when two adjacent sagittal MRIs exhibit a discontinuous body of the meniscus.
Absent bow tie sign is present when two adjacent sagittal MRIs exhibit a discontinuous body of the meniscus.
ANTEATER NOSE2
Introduction and Anatomical Context: Anteater nose is a direct sign of calcaneonavicular coalition. Most common clinical presentation is with anterolateral foot pain due to degenerative osteoarthritis and pes planus.
Etiology: Congenital (most common cause) (Figure 11-2).

Figure 11-2. Anteater nose. (A) Lateral radiograph of the foot shows anteater nose (arrow). (B) Anteater drawing (Used with permission from Arash Tehranzadeh, MD). (C) Oblique radiograph of the foot shows fibrous coalition of calcaneal navicular bones (arrow). (D) CT images of the ankle show fibrous coalition of the calcaneal navicular bones (arrows).
Radiological Findings: Elongated tubular extension on lateral radiograph. This image has been likened to the elongated nose of the anteater. The findings are confirmed on axial CT scan that shows a bone bridge between the calcaneus and the navicular.
Diagnosis: Calcaneonavicular coalition.
Imaging Modality: Radiograph.
PEARLS
![]() Direct sign of calcaneonavicular coalition.
Direct sign of calcaneonavicular coalition.
![]() Confirmed on axial CT images.
Confirmed on axial CT images.
ANTERIOR DRAWER SIGN3
Introduction and Anatomical Context: Anterior cruciate ligament (ACL) runs obliquely within the lateral aspect of the intercondylar notch, attaching to the intercondylar eminence of the tibia distally.
Etiology: Post-traumatic (Figure 11-3).
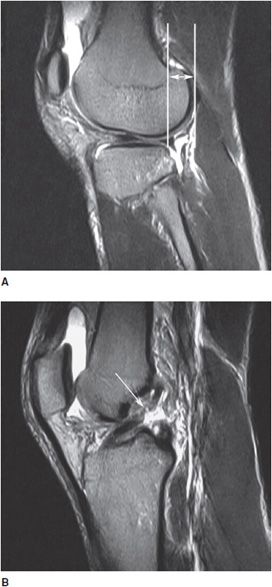
Figure 11-3. Anterior drawer sign. (A) Sagittal T2-weighted image of the knee shows anterior displacement of tibia in relation to femur (double-headed arrow). (B) Sagittal T2-weighted image of the knee shows ACL tear (arrow).
Radiological Findings: Sagittal T2-weighted MRI of the knee with anteriorly displaced/subluxed tibia, relative to femur. Abnormal signal intensity seen in the ACL is suggestive of a tear. This sign is the MR equivalent of the clinically elicited anterior drawer sign indicating ACL teat.
Diagnosis: ACL injury.
Imaging Modality: MRI.
PEARLS
![]() Anterior drawer sign is an indirect evidence of ACL injury. Diagnosis is confirmed by documenting intraligamentous edema, hemorrhage, ligament discontinuity, or contour irregularity.
Anterior drawer sign is an indirect evidence of ACL injury. Diagnosis is confirmed by documenting intraligamentous edema, hemorrhage, ligament discontinuity, or contour irregularity.
BAMBOO SPINE4
Introduction and Anatomical Context: Ankylosing spondylitis is a seronegative, chronic inflammatory disorder that affects the axial skeleton. Changes in the spine (bamboo spine, trolley-track sign and squaring of vertebral bodies) are visible on radiographs and provide adequate diagnosis.
Etiology: Ninety percent of patients with ankylosing spondylitis are HLA-B27 positive (Figure 11-4).

Figure 11-4. Bamboo spine. AP radiograph of the spine.
Radiological Findings: Nearly complete fusion and squaring of the vertebral bodies are noted. Bony outgrowths give a bamboo stalk appearance to the spine.
Diagnosis: Ankylosing spondylitis.
Imaging Modality: Anteroposterior (AP) and lateral radiographs.
PEARLS
![]() Bony outgrowths in ankylosing spondylitis are due to ossification of the annulus fibrosus.
Bony outgrowths in ankylosing spondylitis are due to ossification of the annulus fibrosus.
![]() Bridging osteophytes differentiate ankylosing spondylitis from diffuse idiopathic skeletal hyperostosis (DISH) that has flowing osteophytes, small osteophytes in degenerative joint disease, and large osteophytes in psoriasis and reactive arthritis.
Bridging osteophytes differentiate ankylosing spondylitis from diffuse idiopathic skeletal hyperostosis (DISH) that has flowing osteophytes, small osteophytes in degenerative joint disease, and large osteophytes in psoriasis and reactive arthritis.
BITE SIGN5
Introduction and Etiology: This sign is suggestive of osteonecrosis, avascular necrosis (AVN), or ischemic necrosis. Ischemia of the bone due to a variety of causes can lead to the radiologic sign. Ischemic insult can be due to reduced arterial blood flow or venous insufficiency (Figure 11-5).

Figure 11-5. Bite sign. AP radiograph of the hip shows AVN of the femoral head with its lateral segment missing.
Radiological Findings: A small deformed femoral head is shown with areas of osteolysis and sclerosis. Punched out or gouged out areas of bony destruction, similar to small animal bites, are typical of AVN. This is secondary to repeated steroid injections.
Diagnosis: AVN.
Imaging Modality: Radiograph.
PEARLS
![]() MRI is diagnostic and used for staging of AVN (five stages, 0–IV).
MRI is diagnostic and used for staging of AVN (five stages, 0–IV).
BLADE OF GRASS SIGN6,7
Introduction: Sign suggestive of osteolytic stage of Paget disease.
Etiology: Osteoclastic activity (Figure 11-6).
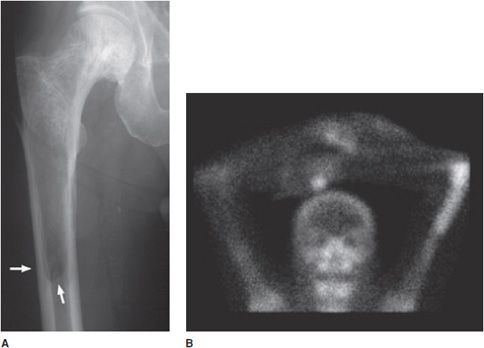
Figure 11-6. Blade of grass sign. (A) AP radiograph of femur. Arrows show advancing age of lesion. (B) Anterior view of bone scan in a different patient shows increased uptake in the distal left humerus due to Paget disease.
Radiological Findings: A well-demarcated radiolucent V-shaped area in the diaphysis. The lucency is extending caudally as a V-shaped or wedge-shaped radiolucent area, likened to a blade of grass.
Diagnosis: Paget disease.
Imaging Modality: Radiograph and bone scan.
PEARLS
![]() Paget disease starts at the epiphysis of the long bones and extends to the metaphysis and diaphysis.
Paget disease starts at the epiphysis of the long bones and extends to the metaphysis and diaphysis.
![]() Paget disease progresses through four phases: lytic, sclerotic, mixed, and malignant phases.
Paget disease progresses through four phases: lytic, sclerotic, mixed, and malignant phases.
![]() Blade of grass sign is seen in osteolytic phase of Paget disease.
Blade of grass sign is seen in osteolytic phase of Paget disease.
![]() High alkaline phosphatase levels are diagnostic for Paget disease in the presence of radiological signs.
High alkaline phosphatase levels are diagnostic for Paget disease in the presence of radiological signs.
BLISTER OF BONE SIGN
Introduction and Anatomical Context: Aneurysmal bone cyst (ABC) is found in long bones, pelvis, and posterior spinal elements.
Etiology: Expansile lytic lesion, primary in most cases. Thirty percent arise within existing bone tumors such as fibrous dysplasia, giant cell tumor, chondroblastoma, or osteoblastoma (Figure 11-7).
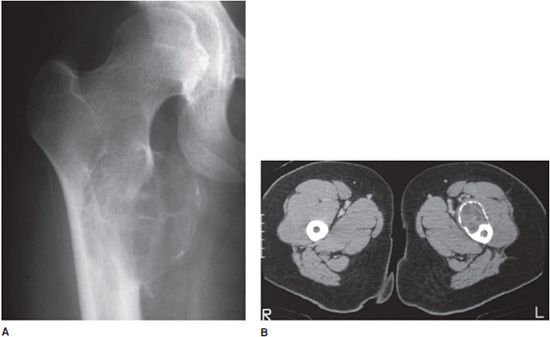
Figure 11-7. Blister of bone sign in aneurysmal bone cyst. (A) AP radiograph of femur with ABC. (B) CT of left femur in different patient with ABC.
Radiological Findings: Frontal radiograph of the right hip and CT scan of the proximal femora on a different patient. Both reveal a cystic and bubbly lesion with fine internal septations. Cortical margin of the lesion is compromised. The bubbly, cystic lesion with a saccular cortical protrusion and multiple internal septae produces a blister of bone sign, highly characteristic of ABC.
Imaging Modality: Radiograph and CT scan.
PEARLS
![]() ABC has no periosteal reaction, unless cyst wall is fractured.
ABC has no periosteal reaction, unless cyst wall is fractured.
![]() ABC has a preserved cortical rim, differentiating from metastases.
ABC has a preserved cortical rim, differentiating from metastases.
![]() ABC is eccentric in location, differentiating it from unicameral bone cyst, which lies centrally in bone metaphysis.
ABC is eccentric in location, differentiating it from unicameral bone cyst, which lies centrally in bone metaphysis.
BONE BRUISE SIGN8–10
Introduction and Anatomical Context: Bone bruise sign in lateral femoral condyle and posterior tibial condyle with anterior drawer sign is suggestive of bone trauma and ACL tear.
Etiology: Trauma leading to edema, hemorrhage, microfracture, and ACL tear (Figure 11-8).

Figure 11-8. Bone bruise sign. (A) Bone edema. (B) Bone edema and ACL tear (arrow).
Radiological Findings: T2-weighted image shows complete ACL tear with mild increase in marrow signal on T2-weighted image in adjacent osseous tissue. The bone bruises as evidenced by increased signal are likely to be caused by impaction of middle and posterior portion of lateral tibial plateau. Signal intensity abnormalities are probably secondary to edema, hemorrhage, and microfracture.
Diagnosis: Indirect sign of bone trauma and ACL tear.
Imaging Modality: Sagittal fluid-sensitive MRI.
PEARLS
![]() Hemorrhage and edema fluid appear hyperintense in the bone marrow on T2-weighted images.
Hemorrhage and edema fluid appear hyperintense in the bone marrow on T2-weighted images.
![]() Bone bruise sign is an indirect sign of trauma and ACL injury.
Bone bruise sign is an indirect sign of trauma and ACL injury.
BONE-IN-BONE SIGN11
Introduction and Anatomical Context: A sign diagnostic of osteopetrosis. The bony change is best visualized on radiograph.
Etiology: Bone-in-bone sign results from failure of osteoclastic activity causing abnormally dense bone that occurs intermittently producing zones of abnormal density alternating with relatively more normal ones (Figure 11-9).

Figure 11-9. Bone-in-bone sign, in osteopetrosis.
Radiologic Findings: Lateral lumbar spine radiograph revealing sclerosis in the superior and inferior portions of the midbody of the vertebra. It gives the appearance of a small replica of the vertebral body inside the normal one, giving a bone-in-bone sign.
Diagnosis: Osteopetrosis.
Imaging Modality: Radiograph.
PEARLS
![]() Bone-in-bone sign is best visualized on radiographs of the spine. It is diagnostic for osteopetrosis (Albers-Schonberg disease).
Bone-in-bone sign is best visualized on radiographs of the spine. It is diagnostic for osteopetrosis (Albers-Schonberg disease).
BOUTONNIERE DEFORMITY12,13
Introduction and Anatomical Context: Boutonniere deformity is the culmination of multiple osseous abnormalities in the hand in rheumatoid arthritis.
Etiology: Inflammatory tear of the central slip of the extensor tendon, which attaches to the middle phalanx (Figure 11-10).
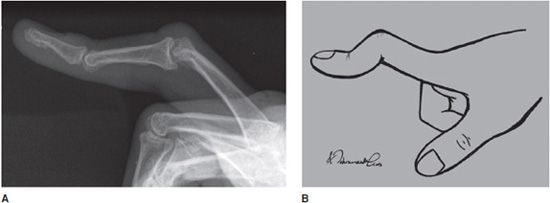
Figure 11-10. Boutonniere deformity. (A) Lateral radiograph of boutonniere deformity. (B) Line drawing (Used with permission from Arash Tehranzadeh, MD).
Radiological Findings: Deformity of little finger noted with hyperextension of distal interphalangeal joints and flexion at proximal interphalangeal joints.
Diagnosis: Rheumatoid arthritis.
Imaging Modality: Radiograph.
PEARLS
![]() Look for chip fracture fragment of the base of the middle phalanx, representing avulsion fracture by central slip of extensor tendon.
Look for chip fracture fragment of the base of the middle phalanx, representing avulsion fracture by central slip of extensor tendon.
BOW TIE SIGN14,15
Normal bow tie is visible on sagittal MRIs in two consecutive images only. Either less or more images showing the bow tie is abnormal.
Etiology: Congenital, normal variant, and more prone to injury (Figure 11-11).
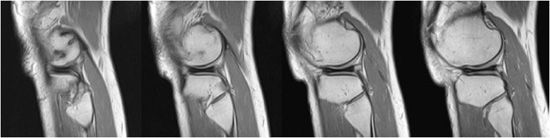
Figure 11-11. Bow tie sign indicating discoid meniscus.
Radiological Findings: Bow tie appearance of the lateral meniscus is seen on 3–5 consecutive, sagittal MRIs. This appearance is consistent with a discoid meniscus.
Diagnosis: Discoid meniscus.
Imaging Modality: MRI.
PEARLS
![]() Excessive bow tie (3–5 consecutive, sagittal MRIs) is a sign of discoid meniscus.
Excessive bow tie (3–5 consecutive, sagittal MRIs) is a sign of discoid meniscus.
![]() Lateral meniscus is less frequently injured as compared with the medial meniscus due to its increased mobility.
Lateral meniscus is less frequently injured as compared with the medial meniscus due to its increased mobility.
![]() Discoid meniscus is a normal variant of lateral meniscus and makes it more prone to injury.
Discoid meniscus is a normal variant of lateral meniscus and makes it more prone to injury.
![]() Discoid meniscus can also be seen in the medial side.
Discoid meniscus can also be seen in the medial side.
BRIM SIGN16
Introduction and Anatomical Context: Brim sign refers to the pelvic brim, also known as the iliopectineal line.
Etiology: Osteoblastic or bone forming stage of Paget disease. Paget disease has four stages: osteolytic, osteosclerotic, mixed, and malignant (Figure 11-12).

Figure 11-12. Brim sign indicating Paget disease (arrows).
Radiological Findings: Patchy sclerosis of right hemipelvis is seen. Thickening of the right pelvic iliopectineal line (brim sign) is visible compared with the left side.
Diagnosis: Paget disease.
Imaging Modality: Radiograph.
PEARLS
![]() Thickening of the iliopectineal line is sign of Paget disease.
Thickening of the iliopectineal line is sign of Paget disease.
![]() Brim sign helps differentiate Paget disease from osteoblastic metastases.
Brim sign helps differentiate Paget disease from osteoblastic metastases.
BUTTON SEQUESTRUM17
Introduction and Anatomical Context: A sequestrum is a small focus of calcification within a radiolucent area.
Etiology: A sequestrum is a devascularized, necrotic piece of bone secondary to a variety of pathological processes (Figure 11-13).

Figure 11-13. Button sequestrum in child with eosinophilic granuloma.
Radiological Findings: Single-slice CT scan of the pelvis with an abnormal lucent area with a sclerotic focus in the left hemipelvis. This sign was originally utilized to describe an unusual radiographic manifestation of eosinophilic granuloma. It is a round, lucent defect with a bony density, or sequestrum, in its center. This is not pathognomonic as other disease entities such as osteomyelitis, tuberculosis, lymphoma, and metastasis can have a similar appearance.
Differential Diagnosis: Eosinophilic granuloma, tuberculosis, lymphoma, metastasis, osteoid osteoma, chondroma, chondroblastoma, and lipoma.
Imaging Modality: CT scan.
PEARLS
![]() Button sequestrum is most commonly seen as a calvarial lesion.
Button sequestrum is most commonly seen as a calvarial lesion.
![]() This sign is not pathognomonic of eosinophilic granuloma, as it is also seen in osteomyelitis.
This sign is not pathognomonic of eosinophilic granuloma, as it is also seen in osteomyelitis.
C-SIGN18
Introduction and Anatomical Context: Subtalar coalition presents most commonly as a flat foot and foot pain. Degenerative osteoarthritic changes are common around the abnormal bone bridge between the talus and the calcaneus.
Etiology: Congenital anomaly (Figure 11-14).

Figure 11-14. C-Sign (arrows) indicating subtalar coalition.
Radiological Findings: Lateral radiograph of the foot revealing a classic C sign that is a C-shaped line formed by the medial outline of the talar dome and the inferior outline of the sustentaculum tali. This sign is a reliable indicator of subtalar coalition on the lateral radiograph and represents the bony bridge between the talar dome and the sustentaculum tali.
Diagnosis: Subtalar coalition.
Imaging Modality: Lateral radiograph.
PEARLS
![]() C-sign is a reliable sign of subtalar coalition on lateral radiograph and represents a bony bridge between the talar dome and the sustentaculum tali.
C-sign is a reliable sign of subtalar coalition on lateral radiograph and represents a bony bridge between the talar dome and the sustentaculum tali.
COCKADE SIGN19
Introduction and Anatomical Context: A cockade is a badge, usually in the form of a rosette, or knot, and generally worn upon the hat.
Etiology: Commonly seen in the proximal femur, fibula, and calcaneus. The lesion is usually asymptomatic and discovered incidentally on imaging (Figure 11-15).

Figure 11-15. Cockade sign indicating intraosseous lipoma.
Radiological Findings: A classic appearance of intraosseous lipoma of the calcaneus is the presence of a well-defined lytic lesion with a central calcification resembling a cockade.
Diagnosis: Intraosseous lipoma.
Imaging Modality: Radiograph.
PEARLS
![]() Intraosseous lipoma presents as an asymptomatic, well-defined radiolucent osseous lesion with a central calcified nidus.
Intraosseous lipoma presents as an asymptomatic, well-defined radiolucent osseous lesion with a central calcified nidus.
CORTICAL RING SIGN20 (SIGNET RING SIGN)
Introduction and Anatomical Context: This sign represents scapholunate dissociation (stage I). It was first described in 1970 in a young patient with bilateral dislocation of the carpal navicular bones.
Etiology: Post-traumatic (Figure 11-16).

Figure 11-16. Cortical ring sign, or signet ring sign, indicating scapholunate dissociation.
Radiological Findings: Multiple images of navicular disorientation with subluxation of the scapholunate joint. The scaphoid bone, seen along its long axis, has a ringed cortex appearance. Cortical ring sign, also known as the signet ring sign, indicates scapholunate dislocation and is caused by the abnormal orientation of the scaphoid bone.
Diagnosis: Rotary subluxation of scaphoid (scapholunate disassociation).
Imaging Modality: Radiograph of wrist.
PEARLS
![]() Cortical ring sign is seen on posteroanterior (PA) view of the wrist, with a signet ring outline of the subluxed scaphoid.
Cortical ring sign is seen on posteroanterior (PA) view of the wrist, with a signet ring outline of the subluxed scaphoid.
COTTON WOOL SIGN21
Introduction and Anatomical Context: Cotton wool sign is a feature of the osteoblastic stage of Paget disease. Osseous lesions are described in four different stages: osteolytic, sclerotic, mixed, and malignant transformation.
Etiology: Unknown (Figure 11-17).
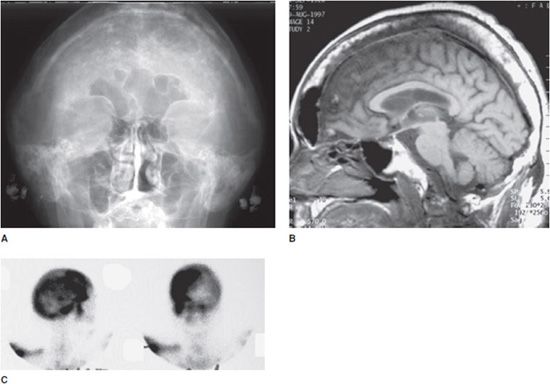
Figure 11-17. Cotton wool sign indicating Paget disease. (A) Radiograph of skull with Paget disease. (B) MRI with Paget disease. (C) Bone scan of skull with Paget disease.
Radiological Findings: Radiograph of the skull reveals a large mottled area of increased radiodensity with small areas of radiolucency within. The MRI of the skull reveals a thickened, enlarged cranium with increase in the marrow space. Two bone scan images also reveal increased activity in the skull, more localized to one side, characteristic to the localized disease seen in Paget disease. This is classic cranial involvement of Paget disease. In the cranium, bone sclerosis may produce circular radiodense lesions in one area, whereas osteoporosis circumscripta is noted elsewhere. In the skull, the common region of involvement is the cranial vault. The osteolytic phase is called osteoporosis circumscripta and appears as multiple geographic, well-demarcated regions of bone resorption that may be mistaken for metastases. Focal radiodensities occur as pagetoid bone is formed. In the quiescent phase, there is a radiodense cotton wool appearance with a thickened vault.
Diagnosis: Paget disease.
Imaging Modality: Radiograph, MRI, and bone scintigraphy.
PEARLS
![]() Although the pathological radiologic osseous changes in the skull mimic osteoblastic metastases, the enlarged calvarium is a good sign of Paget disease.
Although the pathological radiologic osseous changes in the skull mimic osteoblastic metastases, the enlarged calvarium is a good sign of Paget disease.
CRESCENT SIGN22
Introduction and Anatomical Context: Crescent sign is an early diagnostic sign of AVN on radiographs. It signifies a subcortical fracture of the femoral head.
Etiology: Ischemia to the bone due to a wide variety of causes. The basic mechanism is reduced arterial blood flow or venous insufficiency leading to osseous necrosis (Figure 11-18).
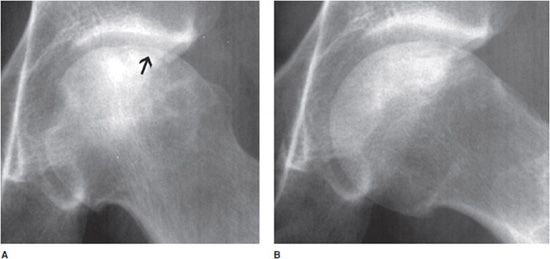
Figure 11-18. Crescent sign indicating AVN. (A) AP radiograph of crescent sign (arrow). (B) Lateral view.
Radiological Findings: A radiograph of a left hip joint, which reveals a thin, curvilinear lucent line parallel to the cortical margin (18A, arrow) of the femoral head. Interruption of the blood supply to the femoral head leads to ischemic necrosis of the marrow and bone that it supplies. Eventually, bone infarcts and insufficiency fractures may ensue. Fractures that occur in the subchondral bone may be recognized by a crescentic lucent zone that separates the fragment from the remainder of the femur.
Diagnosis: AVN.
Imaging Modality: Radiograph and MRI.
PEARLS
![]() Look for a crescentic lucent zone, separating the fracture fragment from the adjacent bone.
Look for a crescentic lucent zone, separating the fracture fragment from the adjacent bone.
![]() MRI is the imaging modality of choice with 100% sensitivity.
MRI is the imaging modality of choice with 100% sensitivity.
CROWDED CARPAL SIGN23
Introduction and Anatomical Context: To understand the carpal dislocation, recall the three carpal arcs. The first arc is a line traced along the proximal carpal row, proximally. The second carpal arc is drawn along the proximal carpal row distally and the third arc is drawn along the distal carpal row, distally. In crowded carpal sign, the first and second arcs are no longer distinct.
Etiology: Post-traumatic (Figure 11-19).

Figure 11-19. Crowded carpal sign indicating volar perilunar dislocation. There is an associated nondisplaced ulnar styloid fracture.
Radiological Findings: Frontal radiograph of the wrist reveals overlap of the distal carpal row with the proximal carpal row. This overriding gives rise to the “crowded carpal” appearance and is a sign specific for volar perilunate dislocation. It is secondary to proximal migration of the distal row of carpal bones during subluxation.
Diagnosis: Volar perilunar dislocation.
Imaging Modality: Radiograph.
PEARLS
![]() Failure to delineate proximal carpal row from the distal carpal row with loss of visualization of first and second carpal arcs indicating volar perilunar dislocation.
Failure to delineate proximal carpal row from the distal carpal row with loss of visualization of first and second carpal arcs indicating volar perilunar dislocation.
CUPID’S BOW SIGN24
Introduction and Anatomical Context: Normal variants are important to recognize to avoid labeling the observation as pathological.
Etiology: Normal variant (Figure 11-20).
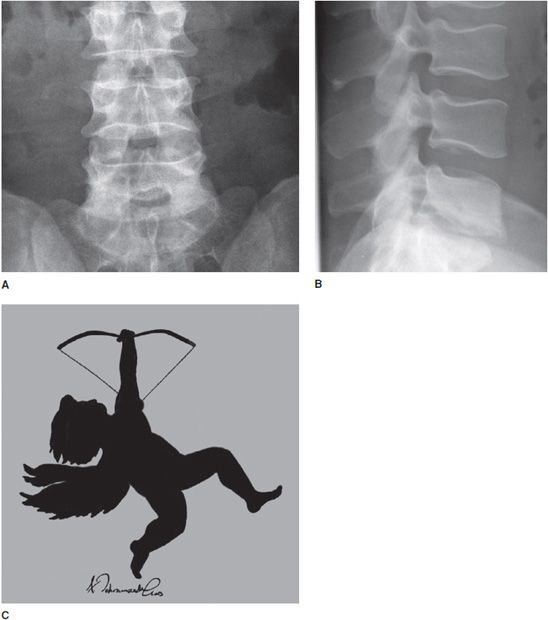
Figure 11-20. Cupid’s bow sign indicating normal variant in endplate of vertebral body. (A) AP view. (B) Lateral view. (C) Cupid drawing (Used with permission from Arash Tehranzadeh, MD).
Radiological Findings: Frontal and lateral radiograph of the lumbar spine with curvature of the inferior endplates of the fourth and fifth lumbar vertebrae, mimicking the curvature of Cupid’s bow aimed cephalad. The unusual, non-flat surface of the inferior endplate is a normal variant, and need not be misinterpreted as inherent osseous abnormality or adjacent pathological process.
Diagnosis: Normal spine.
Imaging Modality: Radiograph.
PEARLS
![]() Normal variant not to be misinterpreted as inherent osseous abnormality or a sign of pathological process.
Normal variant not to be misinterpreted as inherent osseous abnormality or a sign of pathological process.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


