Extrinsic causes
Adhesion
Hernia
Volvulus
Neoplasm (serosal invasion)
Intrinsic causes
Neoplasm (small bowel origin)
Inflammatory bowel disease
Radiation enteritis
Intramural hematoma
Intussusception
Ischemic enteritis
Postoperative stricture
Intraluminal causes
Gallstone
Bezoar
Foreign body
Parasite
13.3.3 Closed-Loop Obstruction
Closed-loop obstruction can be diagnosed if one dilated bowel loop obstructed at a single point, i.e., a closed loop, and another dilated bowel loop proximal to the obstructive site are depicted on CT. Several features can aid in the recognition of a closed-loop obstruction on CT. The beak sign is a beak-shaped configuration of the dilated closed loop toward the obstruction when the bowel is imaged in the longitudinal orientation. Mesenteric vessels of the closed loop appear to be converging toward the point of obstruction forming in radial distribution. The whirled appearance of the mesentery, believed to occur when the afferent and efferent bowel loops rotate around a fixed point to encircle the central vessel, can also be seen, although it is not specific for closed-loop obstruction (Elsayes et al. 2007).
13.3.4 Strangulation
A specific finding of strangulation is the lack of bowel wall enhancement. Delayed or prolonged enhancement of the bowel wall can indicate ischemia. Bowel wall thickening, mesenteric stranding, and ascites are also findings of ischemia, but not specific, as impaired venous outflow by mesenteric torsion or a narrow neck at the obstruction point can also generate these features (Kim et al. 2004; Zalcman et al. 2000). A combination of these features increases the probability of strangulation (Zalcman et al. 2000). Pneumatosis intestinalis accompanying SBO is highly suggestive of bowel ischemia.
13.4 Algorithmic Approach in Diagnosis of SBO
If a high-grade SBO is suspected on simple radiographs or in the clinical setting, MDCT should be taken and evaluation with the following order is recommended: First, we must confirm the SBO by looking for a transition zone and then determine the degree of SBO. Thereafter, the cause of SBO should be identified as SBO by adhesion would not require surgery if not complicated, whereas SBO owing to other conditions such as hernia, cancer, and gallstone usually requires operative management. Finally, the presence of a closed loop or strangulation should be carefully assessed.
In cases of suspicion for low-grade SBO, which sometimes is accompanied by intermittent recurrent nonspecific abdominal pain, enteroclysis or CT enteroclysis is the diagnostic modality of choice.
Summary
1.
MDCT is highly sensitive and specific in the diagnosis of high-grade SBOs, providing important information regarding the cause of obstruction as well as the presence of a closed-loop obstruction or strangulation. Coronal and sagittal reconstruction can be helpful to trace bowel loops and find a transition zone.
2.
SBO is diagnosed when the small bowel is dilated over 3 cm and a transition zone, often immediately distal to the bowel with small bowel feces, is present.
3.
Adhesion is the most common cause of SBO and adhesive ileus is the exclusive diagnosis when no obstructing lesion is identified at the point of obstruction.
4.
Closed-loop obstruction is at risk of strangulation and is mostly caused by mesenteric torsion, volvulus, or hernia. It can be dilated when one dilated bowel loop obstructed at a single point, i.e., a closed loop, and another dilated bowel loop proximal to the obstructive site are depicted on CT.
5.
Lack of bowel wall enhancement is a specific finding for strangulation in SBO. Delayed enhancement, bowel wall thickening, mesenteric congestion, and ascites are possible but not specific findings for strangulation.
6.
MDCT evaluation of SBO should include confirmation of the SBO, identification of its cause, and assessment of the presence of a closed loop or strangulation.
7.
Enteroclysis or CT enteroclysis is the modality of choice in the diagnosis of low-grade obstructions, which challenges the distensibility of the small bowel and exaggerates the effect of mild mechanical obstructions.
13.5 Illustrations: Small Bowel Obstruction
13.5.1 Simple Radiography of Ileal Obstruction
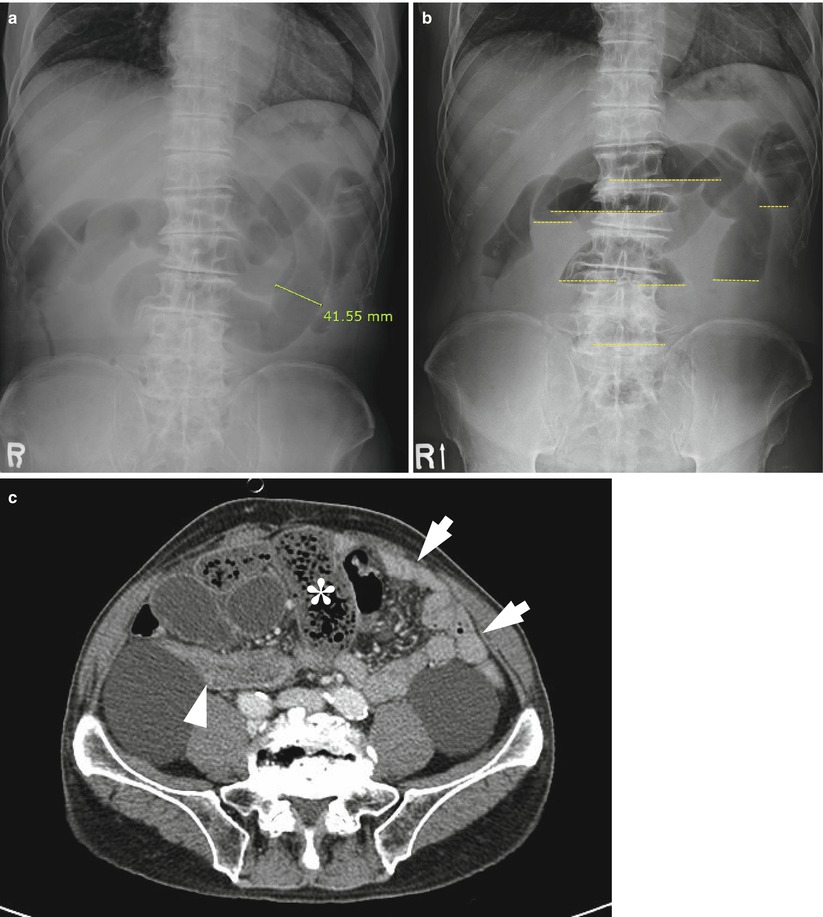
Fig. 13.1
Ileal obstruction in an 84-year-old male patient with a history of surgery for gastric cancer. Supine abdominal simple radiograph (a) shows multiple dilated loops of the small bowel measuring over 4 cm in width with no colonic gas, suggesting small bowel obstruction. The contour of the dilated small bowel loops is smooth with sparse valvulae conniventes, indicating the ileum rather than jejunum. Erect abdominal simple radiograph (b) shows multiple air–fluid levels at different heights (yellow dotted lines). Axial CT scan (c) shows a dilated small bowel with fluid and small bowel feces (asterisk) in the right abdomen, collapsed ascending colon (arrowhead), and collapsed jejunal loops (arrows) in the left abdomen which has not yet dilated
13.5.2 String of Pearls Sign on Plain Radiograph
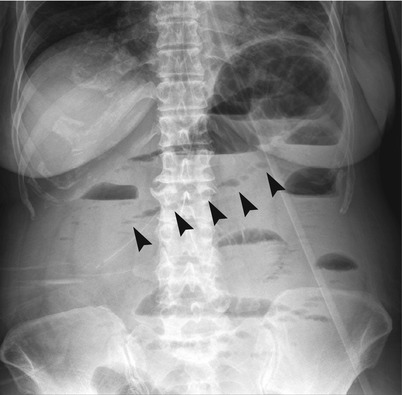
Fig. 13.2
String of pearls sign in a 56-year-old female patient with small bowel obstruction. Erect abdominal simple radiograph demonstrates a row of small air bubbles (arrowheads), which represent air trapped between the valvulae conniventes. Note the prominent valvulae conniventes in the dilated jejunal loops in the left upper quadrant
13.5.3 Schematic Drawing of the Degree of Small Bowel Obstruction
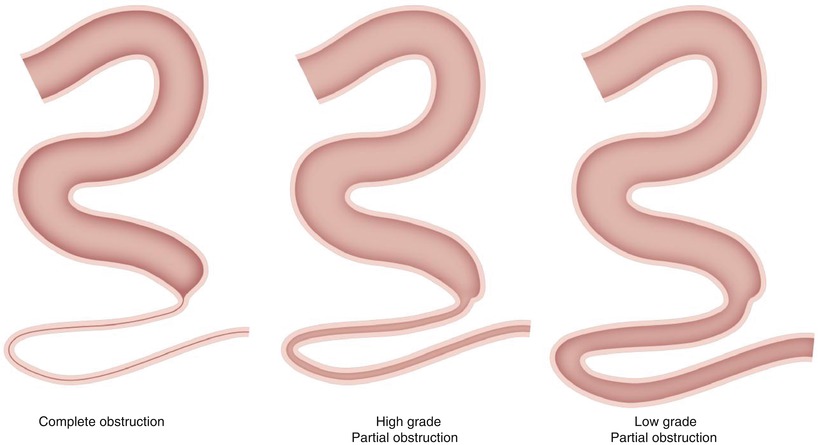
Fig. 13.3
Schematic drawing of the degree of small bowel obstruction. Complete obstruction is characterized by a distended bowel associated with failure to pass bowel content at the site of the obstruction as well as the presence of a collapsed distal bowel. In incomplete partial obstruction, bowel loops distal to the transition zone have a certain amount of intraluminal content. In high-grade partial obstruction, the discrepancy of the luminal diameter between the proximal and distal segments is large, sometimes defined as a difference in luminal diameter of more than three times. In low-grade partial obstruction, the discrepancy is not prominent
13.5.4 Simple Adhesive Ileus with Typical Small Bowel Feces Sign
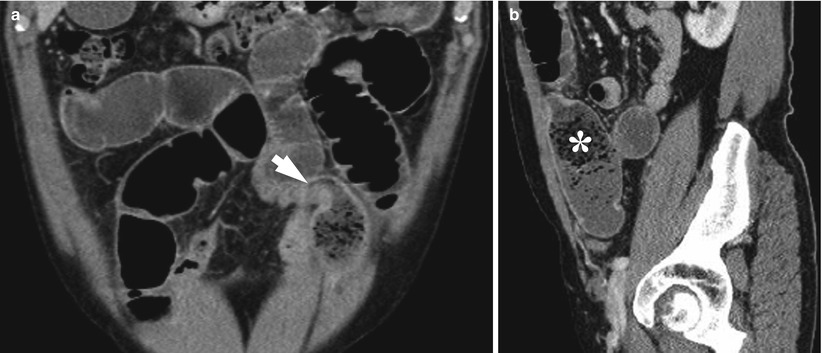
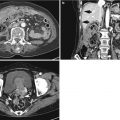
Fig. 13.4
Simple adhesive ileus with typical small bowel feces sign in a 66-year-old male patient. Coronal reformatted image (a) demonstrates a sharp transition zone (arrow) at the site of the adhesion abutting the abdominal wall. On sagittal image (b), the typical small bowel feces sign (asterisk) and presence of particulated materials containing air bubbles visible in the proximal dilated segment of the bowel are noted
13.5.5 Closed-Loop Obstruction Due to Adhesive Bands
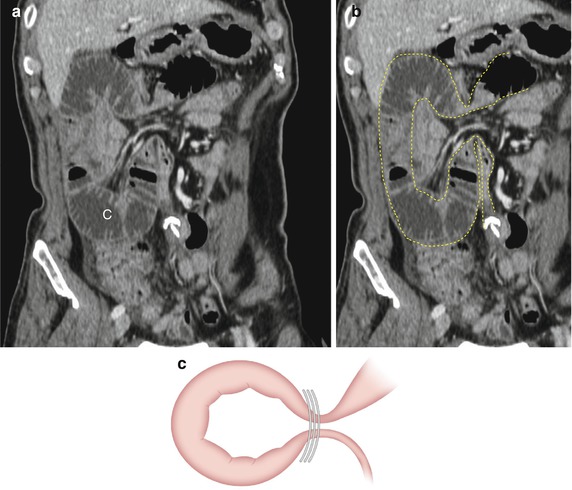
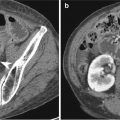
Fig. 13.5
Closed-loop obstruction due to adhesive bands in a 66-year-old male patient with a history of surgery for rectal cancer. Curved MPR image (a) demonstrates two adjacent transition zones (empty arrows) with extraluminal compression by fat tissue, suggesting an adhesive band. To the right of the obstruction site, a C-shaped dilated closed loop (“C”) is noted, whereas a dilated proximal loop with gas (“P”) and a collapsed distal bowel (solid arrow) located left of the obstruction are noted. This patient underwent surgery and the adhesive band between the omentum and small bowel was confirmed. A schematic drawing of this case (b) and a diagram of the closed loop due to adhesive bands (c) are shown
13.5.6 Closed-Loop Obstruction Owing to Small Bowel Volvulus
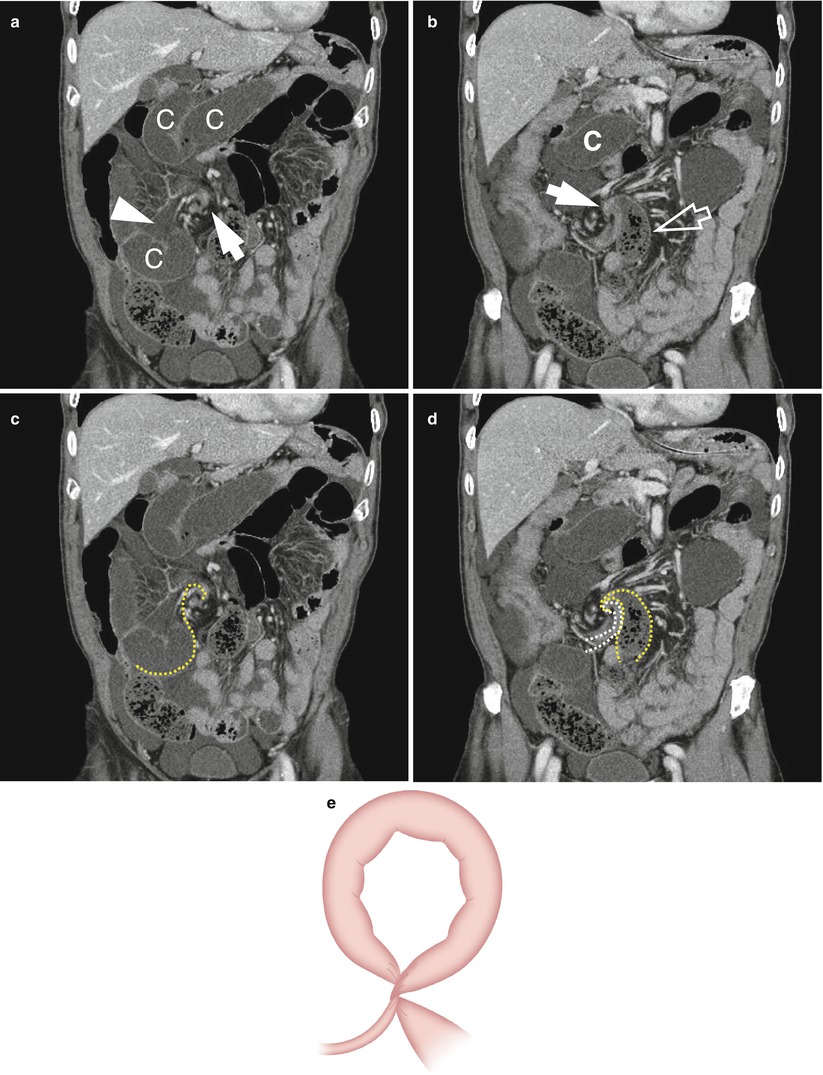
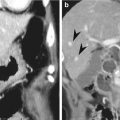
Fig. 13.6




Closed-loop obstruction owing to small bowel volvulus in an 84-year-old male patient. Coronal reformatted images (a, b) show whirled mesentery (solid arrows) in the right paramedian abdomen, with subsequent dilated closed loops (“C”) and a dilated proximal small bowel (empty arrow) exhibiting the small bowel feces sign. Note the prominent mesenteric congestion (arrowhead) at the closed loop and ascites, which are possible findings for strangulation. On the same images (c, d), the scheme of the bowel configuration was drawn (yellow and white dotted lines). A schematic diagram of the closed loop due to volvulus (e) is presented
Related posts:
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
