patient’s age, a displacement of the normal positions of the fat pads of the elbow also provides a useful diagnostic clue to the presence of a fracture. Normally, the posterior fat pad, which lies deep in the olecranon fossa, is not visible on the lateral view. When it becomes visible and the anterior fat pad appears displaced—the positive fat-pad sign (Fig. 6.11; see Fig. 4.35)—demonstration of the fracture line should be undertaken.
 FIGURE 6.1 Osseous structures of the elbow. Anterior and posterior views of the distal humerus and the proximal radius and ulna. |
 FIGURE 6.2 Muscles of the elbow. Anterior and posterior views of the muscles of the elbow joint. |
 FIGURE 6.3 Ligaments of the elbow. Medial and lateral views of the ligaments of the elbow joint. |
 FIGURE 6.4 Anteroposterior view. (A) For the anteroposterior view of the elbow, the forearm is positioned supine (palm up) on the radiographic table, with the elbow joint fully extended and the fingers slightly flexed. The central beam is directed perpendicularly toward the elbow joint. (B) The film in this projection demonstrates the medial and the lateral epicondyles, the olecranon fossa, the capitellum, and the radial head. The coronoid process is seen en face, and the olecranon overlaps the trochlea. |
 FIGURE 6.5 Carrying angle. The angle formed by the longitudinal axes of the distal humerus and the proximal ulna constitutes the carrying angle of the forearm. Normally, there is a valgus angle of 15 degrees. |
 FIGURE 6.6 Ossification centers of the distal humerus. The secondary centers of ossification of the distal humerus usually appear in the following order: the capitellum at 1 to 2 years of age, the medial epicondyle at 4 years of age, the trochlea at 8 years of age, and the lateral epicondyle at 10 years of age. |
 FIGURE 6.7 Fracture of the medial epicondyle. Displacement of the ossification center of the medial epicondyle secondary to fracture (A) and (B) may mimic the normal appearance of the ossification center of the trochlea (C). The orange areas represent unossified cartilage which is not visualized on the radiographs. |
 FIGURE 6.8 Lateral view. (A) For the lateral projection of the elbow, the forearm rests on its ulnar side on the radiographic cassette, with the joint flexed 90 degrees, the thumb pointing upward, and the fingers slightly flexed. The central beam is directed vertically toward the radial head. (B) The film in this projection demonstrates the distal shaft of the humerus, the supracondylar ridge, the olecranon process, and the anterior aspect of the radial head. The articular surface and posterior aspect of the radial head are not well demonstrated on this view because of overlap by the coronoid process. The capitellum is also obscured by the overlapping trochlea. |
 FIGURE 6.9 Supracondylar fracture. (A) Lateral radiograph of the elbow joint in a 3-year-old child shows the normal hockey-stick appearance of the distal humerus. (B) Loss of this configuration, as seen in this radiograph in a 3.5-year-old girl who sustained trauma to the elbow 4 weeks before this examination, serves as an important landmark in recognizing supracondylar fracture of the distal humerus. Note also that the anterior humeral line falls anterior to the capitellum, indicating an extension injury (see Fig. 6.10). |
 FIGURE 6.10 Landmarks of the elbow joint. In children, the normal position of the capitellum relative to the distal humerus and the proximal radius is determined by the portions of the capitellum intersected by two lines: Line (a) coincident with the longitudinal axis of the proximal radius passes through the center of the capitellum and line (b) parallel to the anterior cortex of the distal humerus intersects the middle third of the capitellum. Disruption of this relation indicates the possible presence of an abnormality (see Figs. 6.9B and 6.25B). |
 FIGURE 6.11 Fat-pad sign. Lateral radiograph of the elbow joint shows positive anterior (arrow) and posterior (curved arrow) fat-pad sign. Open arrow points to the subtle fracture of the radial head. |
 FIGURE 6.12 Radial head-capitellum view. (A). For the radial head-capitellum projection of the elbow, the patient is seated at the side of the radiographic table, with the forearm resting on its ulnar side, the elbow joint flexed 90 degrees, and the thumb pointing upward. The central beam is directed toward the radial head at a 45-degree angle to the forearm. (B) The film in this projection shows the radial head projected ventrad, free of overlap by the coronoid process, which is also well demonstrated. This projection is also effective in evaluating the capitellum and the humeroradial and humeroulnar articulations. |
these structures that may be obscure on other projections (see Figs. 6.27, 6.28, and 6.34).
 FIGURE 6.13 Arthrography of the elbow joint. (A) For arthrographic examination of the elbow, the patient’s forearm is positioned prone on the radiographic table, with the joint flexed 90 degrees and the fingers lying flat. The joint is entered from the lateral aspect between the radial head and the capitellum, and under fluoroscopic control, 2 mL of positive contrast agent (60% diatrizoate meglumine) and 8 to 10 mL of room air are injected into the radiocapitellar joint. (The red dot marks the point of needle entrance.) Conventional radiographs or tomograms may then be obtained in the standard projections (see Figs. 6.14 and 6.42). (B,C) On the elbow arthrogram, one can distinguish anterior, posterior, and annular recesses of the joint capsule. The articular cartilage of the radial head and capitellum is also well demonstrated. |
sections) provide an ideal plane for the evaluation of the olecranon fossa and the space between the trochlea and the olecranon process posteriorly, as well as the radius and the capitellum, and the trochlea and the coronoid process anteriorly. Axial scans through the flexed elbow also allow additional demonstration of the proximal radius in its long axis.
 FIGURE 6.14 Arthrotomography of the elbow joint. A trispiral section through the ulnar-trochlear articulation (A) demonstrates the coronoid recess (arrow) and through the radiocapitellar articulation (B) demonstrates the annular (periradial) (arrow), anterior (curved arrow), and posterior (open arrow) recesses of the joint capsule. |
 FIGURE 6.15 CT-arthrography of the elbow. Postarthrography coronal CT scan of the elbow joint clearly demonstrates the annular recess and the outline of the lateral extension of the joint capsule. The articular cartilage is also well demonstrated. |
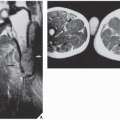
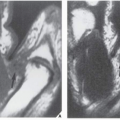
 FIGURE 6.16 Normal MRI anatomy of the elbow joint. On the coronal section (A), note the anatomic relationship of bony, muscular, and tendinous structures. On the sagittal sections (B) and (C), the muscular structures (brachialis muscle, anconeus muscle), tendons (triceps tendon, biceps tendon), and bones (distal humerus, olecranon process, and radial head) are well demonstrated. (From Beltran J, 1990, with permission.) |
 FIGURE 6.17 MRa of the elbow. (A) Coronal T1-weighted fat-suppressed image shows the anterior band of the ulnar collateral ligament (arrow) and the radial collateral ligament (curved arrow). The joint is outlined by a bright contrast agent. C, capitellum; T, trochlea; RH, radial head. (B) Sagittal T1-weighted fat-suppressed image obtained through the medial part of the elbow joint shows anterior (arrow) and posterior (open arrow) recesses. T, trochlea; O, olecranon; BM, brachialis muscle; TM, triceps muscle. (C) Sagittal T1-weighted fat-suppressed image obtained through the lateral part of the elbow joint shows attachment of the joint capsule to the proximal radius (arrow) and its posterior extent (open arrows). C, capitellum; RH, radial head. |
TABLE 6.1 Checklist for Evaluation of MRI and MRa of the Elbow | |||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||
TABLE 6.2 Standard and Special Radiographic Projections for Evaluating Injury to the Elbow | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 6.3 Ancillary Imaging Techniques for Evaluating Injury to the Elbow | |||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||
Related posts:
 Miscellaneous Metabolic and Endocrine Disorders
Miscellaneous Metabolic and Endocrine Disorders
 Benign Tumors and Tumor-like Lesions III: Fibrous, Fibroosseus, and Fibrohistiocytic Lesions
Benign Tumors and Tumor-like Lesions III: Fibrous, Fibroosseus, and Fibrohistiocytic Lesions
 Upper Limb III: Distal Forearm, Wrist, and Hand
Upper Limb III: Distal Forearm, Wrist, and Hand
 Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
 Upper Limb III: Distal Forearm, Wrist, and Hand
Upper Limb III: Distal Forearm, Wrist, and Hand
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


