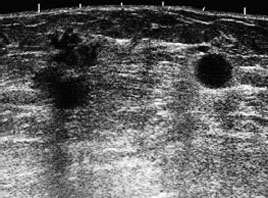
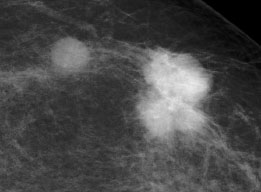
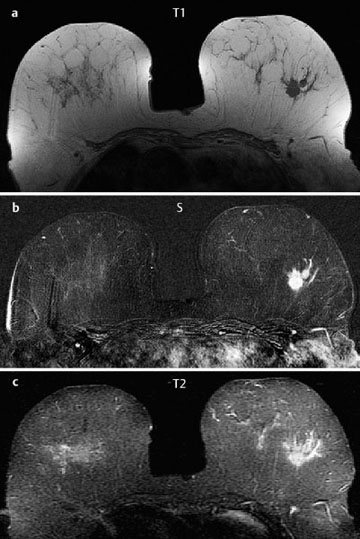
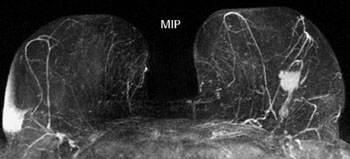
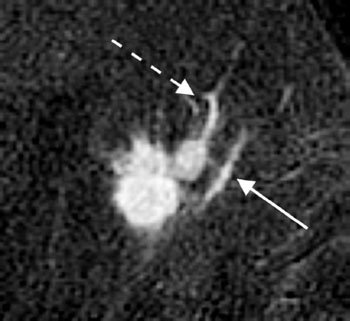
Case 1 Indication: Palpable mass in the left breast, upper outer quadrant, discovered 8 weeks prior to examination. History: Unremarkable. Risk profile: No increased risk. Age: 78 years. Fig. 1.1 Sonography of the left breast. Panoramic view. Dense, mobile mass of diameter 2 cm in the upper outer quadrant of the left breast. Ptosis of the left breast. Fig. 1.2a,b Digital mammography, MLO view. Fig. 1.3 Magnification view of the upper outer quadrant of the left breast, CC view. Fig. 1.4a—c Contrast-enhanced MRI of the breasts. Fig. 1.5 Contrast-enhanced MR mammography. Maximum intensity projection. Fig. 1.6a, b Signal-to-time curve. Please characterize the ultrasound, mammography and MRI findings. What is your preliminary diagnosis? What are your next steps? Corresponding to the palpable mass, ultrasound demonstrates a suspect lobulated lesion with predominantly ill-defined borders and a hyperechoic marginal area. This lesion disturbs ligaments and leads to retraction of the surrounding parenchyma. Close to this lesion, ultrasound shows a pathologically enlarged lymph node. Assessment: US BI-RADS left 5. Mammography shows symmetric lipomatous breast tissue of ACR type 1. There are no pathological findings in the right breast. In the upper outer quadrant of the left breast, there is a lobulated mass (2 cm diameter) with ill-defined borders. A bridge of dense tissue is seen between the lesion and a prepectoral lymph node about 2 cm away. There is a further partially visible, enlarged lymph node in the left upper axilla. No microcalcifications are detectable (BI-RADS right 1/left 5). PGMI: G (the inframammary fold was not clearly discernible). MRI shows a mass 2 cm in diameter in the upper outer quadrant of the left breast. There is a second small nodule nearby. After administration of contrast the tumor shows marked initial enhancement, followed by washout. There is ductal enhancement extending from the primary tumor to the lateral parts of the left breast (Fig. 1.7; arrow). MIP demonstrates pathological enhancement of the prepectoral lymph node as well as the bridge like connection between tumor and lymph node. Fig. 1.7 Contrast-enhanced MR mammography. Magnification view of the left breast, upper outer quadrant. Caution: Other linear structures with increased vascularization correlate with contrast-enhanced veins (broken arrow). MRI Artifact Category: 2 MRI Density Type: 1
Clinical Findings



Ultrasound
Mammography
MR Mammography
MRM score | Finding | Points |
Shape | lobulated | 0 |
Border | ill-defined | 1 |
CM Distribution | inhomogeneous | 1 |
Initial Signal Intensity Increase | strong | 2 |
Post-initial Signal Intensity Character | wash-out | 2 |
MRI score (points) |
| 6 |
MRI BI-RADS |
| 5 |
 Preliminary Diagnosis
Preliminary Diagnosis
Invasive breast cancer of the left breast with lymph node metastases, stage T2. No differential diagnosis.
Clinical Findings | right 1 | left 5 |
Ultra sound | right 1 | left 5 |
Mammography | right 1 | left 5 |
MR Mammography | right 1 | left 5 |
BI-RADS Total | right 1 | left 5 |
Next step according guidelines
US-guided core biopsy of the palpable mass in the left breast
Performed step (departing from guidelines)
Due to the age of the patient and the clear findings in all imaging modalities, and in response to the patient’s own request, a US-guided core biopsy for preoperative histopathological diagonsis was not performed. The tumor was examined histopathologically following mastectomy.
Histology
Medullary carcinoma of the left breast.
MC pT2 (2.5 cm), pN1 a (2/18), G2.



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


