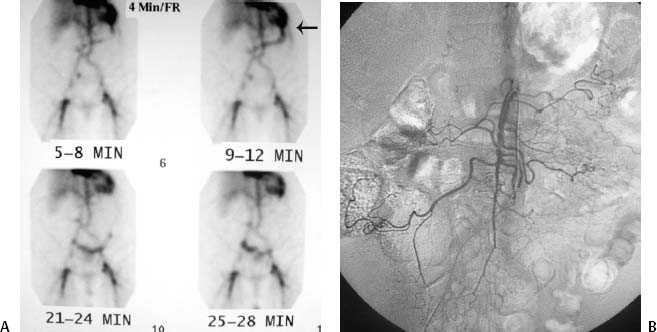
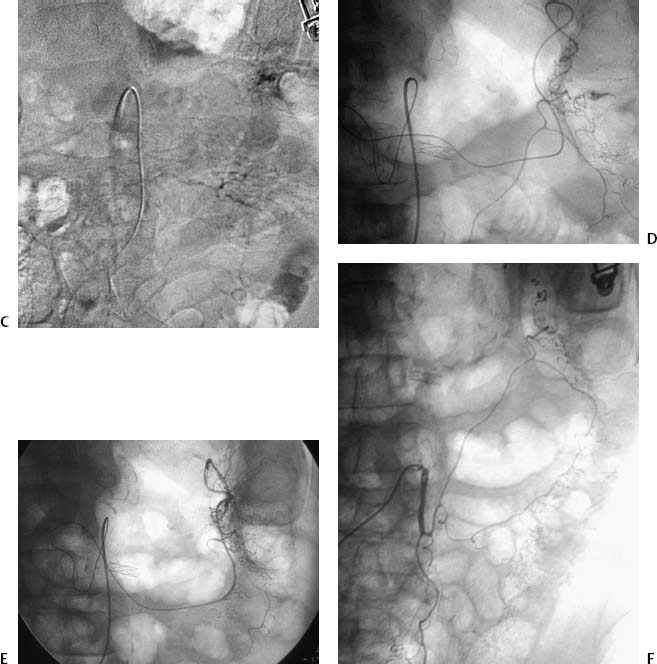
CASE 1 A 56-year-old female presented to the emergency department with bright red blood per rectum. She received two units of packed red blood cells (RBC) and was sent for a nuclear medicine-tagged red blood cell study for further evaluation. Figure 1-1 Microcoil embolization of left colonic hemorrhage. (A) Nuclear scintigraphy shows bleeding from the left colon (arrow). (B) Superior mesenteric angiogram in the early arterial phase shows no obvious bleeding. (C) Superior mesenteric angiogram in early venous phase shows extravasated contrast at the splenic flexure of the colon (large black arrow). (D) Angiogram via 3F microcatheter shows active bleeding at the splenic flexure of the colon. (E) Angiogram after microcoil embolization through microcatheter shows no further bleeding. Note microcoils (white arrow). (F) Final inferior mesenteric angiogram shows arrest of hemorrhage. Note microcoils (long arrow). A tagged RBC study demonstrated uptake with migration in the expected region of the left colon near the splenic flexure (Fig. 1-1). The patient was then referred urgently for mesenteric angiography. The right common femoral artery was punctured using the Seldinger technique and a 5-French (F) sheath was inserted. The superior mesenteric artery (SMA) was catheterized using an RC-1 catheter (Boston Scientific, Natick, Massachusetts), and angiography was performed showing contrast extravasation from a middle colic branch supplying the splenic flexure. Colonic hemorrhage at splenic flexure. Puncture needle 5F vascular sheath 5F mesenteric catheters (RC-1, RIM, VS-1) 0.035” conventional and hydrophilic soft-tipped guidewires 3F microcatheter with guidewire Contrast material Platinum microcoils (2 × 20, 3 × 30 mm) Polyvinyl alcohol particles (500 to 700 microns) A 3F microcatheter was advanced through the SMA catheter. The bleeding vessel was catheterized superselectively using the microcatheter. Superselective angiography revealed extravasation indicating active hemorrhage. Several microcoils were deployed along the mesenteric border of the colon in the marginal artery to enable hemostasis. The patient stopped bleeding and was discharged the following afternoon.
Clinical Presentation
Radiologic Studies
Nuclear Scintigraphy
Angiography
Diagnosis
Treatment
Equipment
Superselective Embolization
Discussion
Background
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


