1 Thoracic Wall
Introduction
The thoracic (chest) wall is composed of the rib cage, inner and outer muscles, vessels, lymphatics, fascia, and skin. The rib cage is formed by the ribs, costal cartilages, sternum, and thoracic vertebrae. The thoracic inlet is the passage of the trachea, aortic arch arteries, major veins, and lymphatics. The outlet of the thorax is covered by the diaphragm. The thoracic wall protects the heart, major vessels, lungs, and part of the liver and spleen. It provides a flexible skeletal framework to promote respiratory movements, stabilize the actions of the diaphragm, shoulders, and arms. 1 The chest also provides attachments for the proper function of the neck, chest, and upper abdomen muscles. Chest wall dysfunction is associated with significant complications and rapid life-threatening consequences. Knowledge of the anatomy and function of the thoracic wall is essential in imaging interpretation of the chest pathologies. This chapter focuses on chest anatomy and function, with emphasis on common anatomical variants and pathologies.
Embryology
The somitic mesoderm gives rise to the osseous parts of the ribs and vertebrae. The lateral plate mesoderm is where the sternum and appendicular (limb) skeleton develop whereas the cranial neural crest forms the branchial arch, craniofacial bones, and cartilage. 2
Ossification of the mesoderm occurs in two forms. In the first form, ossification occurs directly within preexisting mesenchymal tissue. This type of ossification is called intramembranous which is common in flat bones (e.g., skull). In the second form, the mesenchymal progenitor cells differentiate into the chondrocytes that form hyaline cartilage and ossification occurs within hyaline cartilage. The second type is called endochondral ossification.
The rib primordium is identifiable in the fifth week of development (Fig. 1‑1). These primordial ribs are aligned ventrolaterally, next to the intervertebral disks, into the hypaxial muscle anlagen. The first seven to eight ribs increase in length, while the length of the last four ribs will be progressively shorter from cranial to caudal. By the seventh week, the first eight ribs bend toward the sternal anlagen. The primary rib ossification center is located near the angle of the ribs and mostly become cartilaginous during weeks 13 to 14 of development and later become ossified. At birth most ribs are ossified. Secondary rib ossification centers appear later at puberty. The ventral ends of the ribs remain cartilaginous, the so-called “costal cartilage.” Later in life partial calcification of the costal cartilages is a universal finding.
The sternal primordium is first identifiable at 6.5 weeks of development as three mesenchymal condensations; a single median center known as “presternal” and a pair of lateral centers known as “sternal bars.”
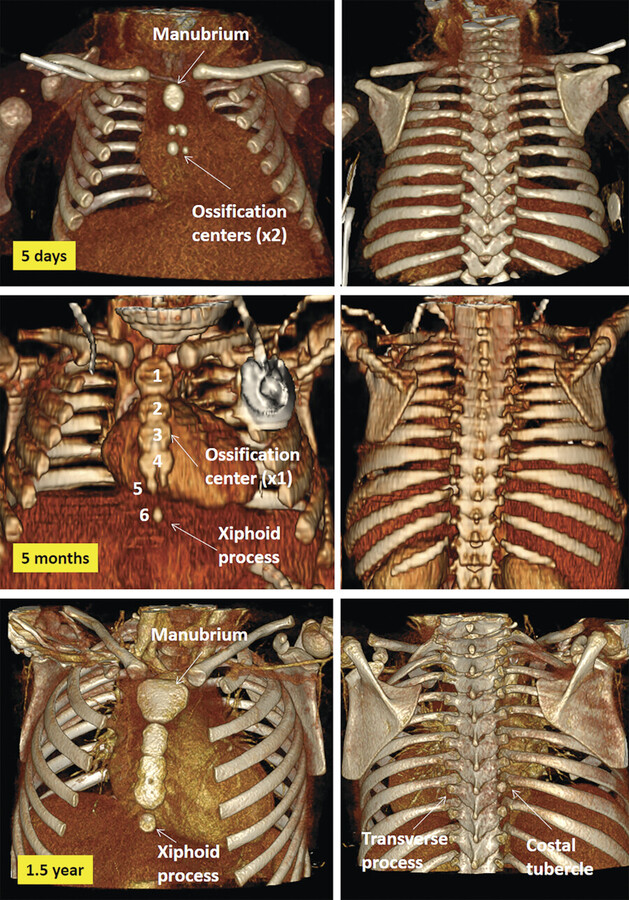
The presternal condensation forms the sternal manubrium in the seventh week which extends to the second rib in the eighth week. At the seventh week, the paired sternal bars move from the lateral to the inferior aspect of the manubrial primordium. By eight weeks, the sternal bars extend to the level of the seventh rib and begin to align with the manubrium and fuse with each other. The medial fusion of the sternal bars continues to the level of the fifth rib in the ninth week but remains bifid more caudally until fusion is complete in the 10th week to form the cartilaginous sternum. Sternal ossification centers appear from superior to inferior direction before birth except in the xiphoid process which appears during childhood (Fig. 1‑2). In the neonate, the manubrium contains one main ossification center. Ossification of the body of the sternum occurs shortly after birth. The number and position of ossification centers vary. By the end of the first year, most individuals have three to four center of ossifications in the sternal body separated from each other by cartilaginous bands (Fig. 1‑2). These bands are connected to the end of the costal cartilages. Union of the bands begins at about puberty and continues to the age of 25 craniocaudally (Fig. 1‑2 , Fig. 1‑3). The xiphoid process may remain ununited in some individuals.
All muscles develop from the somitic dermomyotomes. Muscles of the chest and abdominal wall are grouped into the hypaxial (ventral group) and epaxial (dorsal group) muscles based on their different innervations by the ventral and dorsal rami, respectively. At 5 weeks of development, separate epaxial and hypaxial myotomal compartments with separate dorsal and ventral spinal nerves will become identifiable (Fig. 1‑1).

The muscle cells of the ventral body wall develop from the hypaxial half of the dermomyotome and are innervated by the ventral branch of the spinal nerves. The differentiation of the single band of hypaxial muscle into separate layers will be apparent at the end of the sixth week. At this time the external oblique, internal oblique, transverse abdominal, and rectus abdominal muscles will differentiate. The intercostal and all abdominal wall muscles become identifiable as separate entities from the common myotomal band at 6 to 6.5 weeks of development. The epaxial myotomal compartment will form the paraspinal muscles.
Bony Thorax
The thoracic skeleton is an osteocartilaginous framework that surrounds and protects the thoracic viscera and supports the mechanical function of ventilation. The bony thorax is formed by the sternum anteriorly and the thoracic vertebrae posteriorly, interconnected by the 12 paired ribs and their costal cartilages 3 , 4 , 5 , 6 (Fig. 1‑2 , Fig. 1‑3 , Fig. 1‑4).

Ribs
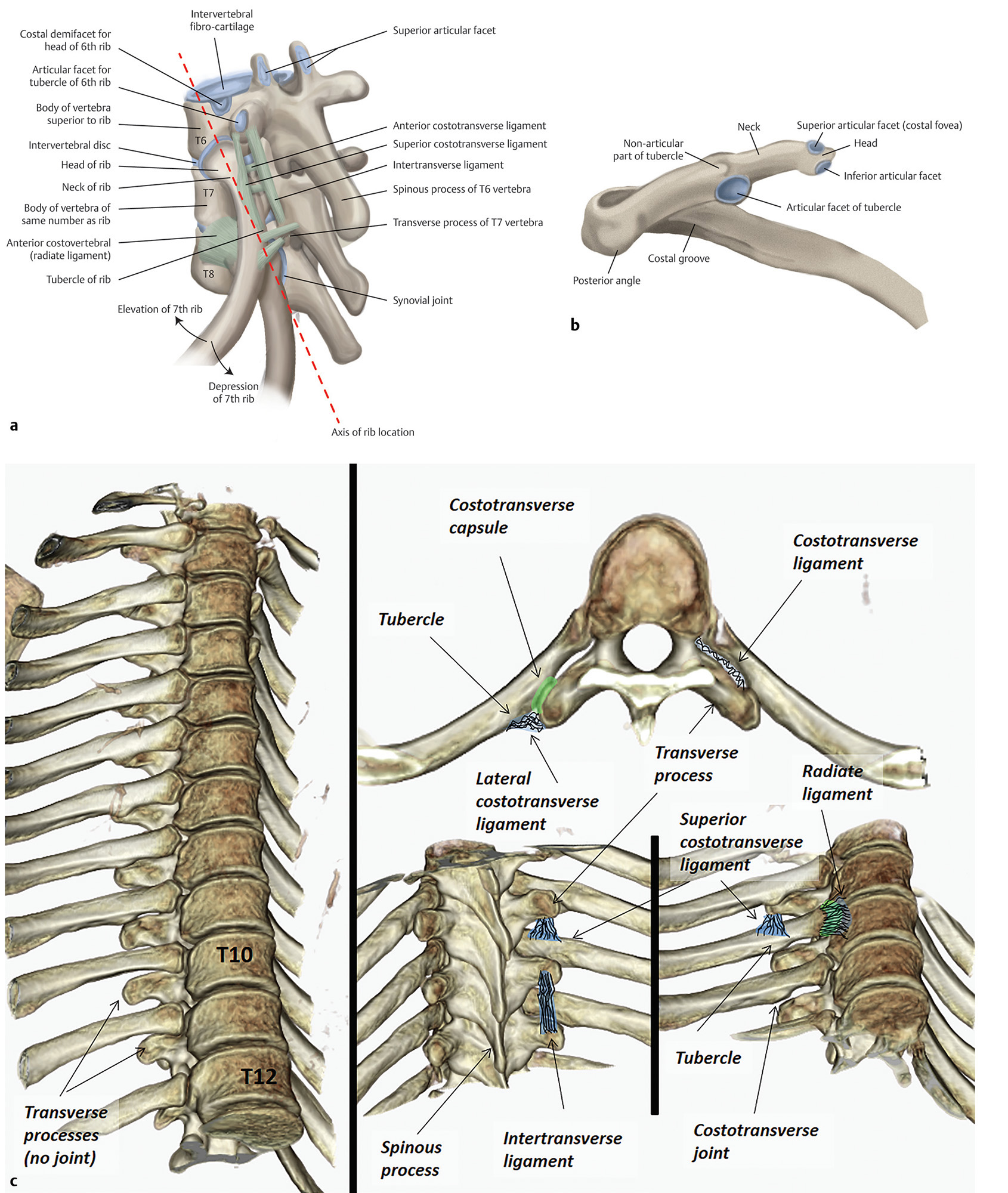
The upper seven ribs directly articulate to the sternum by costal cartilages. These first seven ribs are called true ribs. In contrast, the costal cartilages of the 8th, 9th, and 10th ribs connect to each other and with the 7th costal cartilage. These ribs are called false ribs. The 11th and 12th ribs are called floating because they have no anterior attachment. Each rib consists of a head, a neck, a shaft, and a costal cartilage (Fig. 1‑5). The head and neck are close to the spine. At costovertebral junctions, the rib’s head is articulated by two synovial demifacet joints to the posterolateral aspect of two vertebral bodies at the intervertebral disks (Fig. 1‑5). The inferior rib facet is joined with vertebral body at the same number. Exceptions are the first, 11th, and 12th ribs in which there is a single articular facet (Fig. 1‑6). The 10th rib is sometimes floating with a single costovertebral facet. The costovertebral junctions are covered with a capsule and reinforced by the radiate ligament (Fig. 1‑5).
The neck of the rib spans between the head and the tubercle. The neck of the rib, at its distal end where the rib tubercle is located, articulates with the transverse process of the numerically corresponding vertebra (Fig. 1‑5; Fig. 1‑6). The costotransverse joint is a synovial joint covered with a capsule and strengthened by the costotransverse ligament complex (Fig. 1‑5). It is absent at the 10th,11th, and 12th ribs. The costotransverse ligament complex consists of the main costotransverse ligament, lateral costotransverse ligament, and superior costotransverse ligament (Fig. 1‑5). Other associated ligaments include ligament of the neck of the rib, ligament of tubercle of the rib, and an accessory ligament (Fig. 1‑5).
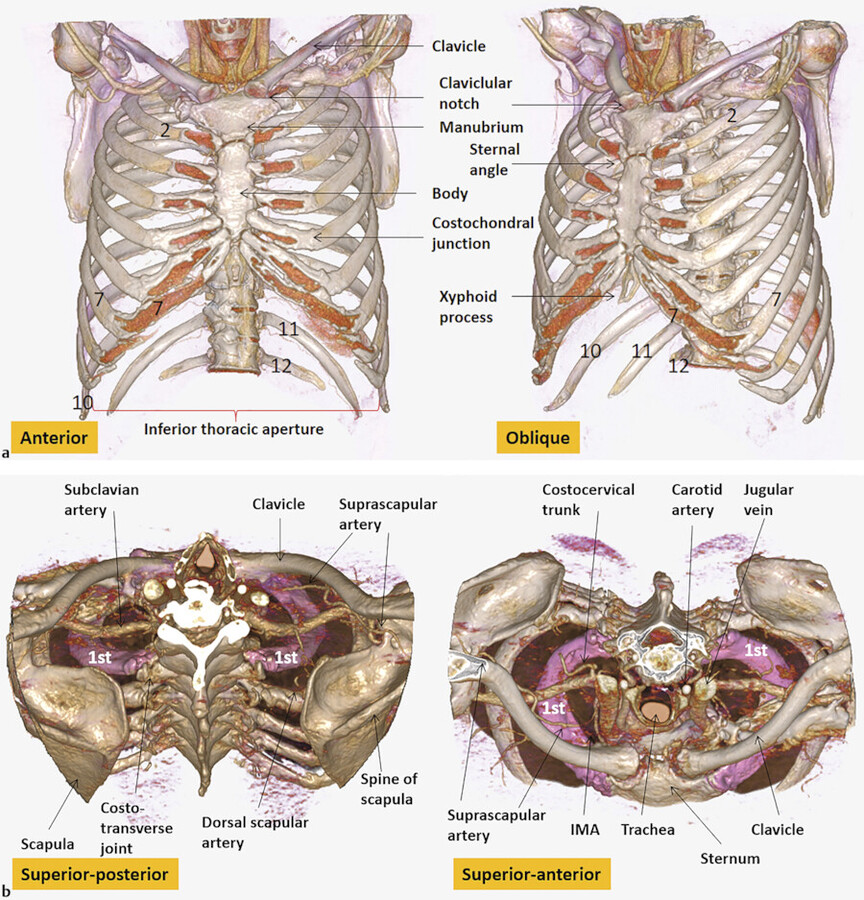
Secondary ossification centers appear for the head and tubercle of the rib at puberty. The 11th and 12th ribs have no necks or tubercles. The shaft of the rib starts distally to the costotransverse joint. The ribs curve and slope inferiorly such that their sternal ends and the costal cartilages are more caudal than their dorsal ends. The ribs are connected with each other by the intercostal muscles. Intercostal vessels and nerves run in the intercostal spaces. The first rib is an important rib that protects the thoracic inlet structures (Fig. 1‑3). The first rib is the shortest, broadest, and most curved of all ribs with no significant move during quiet respiration. From anterior to posterior the following muscles attach to the first rib; the subclavius, anterior scalene, first digitation of the serratus anterior, and middle scalene (Fig. 1‑7). The serratus anterior, serratus posterior superior, and posterior scalene muscles attach to the second rib. The longissimus and iliocostalis muscles attach to the posterior ribs. The iliocostalis muscles attach to the rib angle where rib starts to bend and the longissimus muscles attach between the tubercle and angle.
The rib cage morphology changes with age and sex. At birth, ribs are oriented horizontally but gradually become sloped. From birth through adolescence, the rib cage increases in size and ribs move inferiorly (Fig. 1‑2 , Fig. 1‑3). There is also a decrease in thoracic kyphosis. From young adulthood into elderly age, there will be increasing kyphosis and more horizontal course of the ribs relative to the spine. 7 Additional age-related increase size of the upper thorax is seen compared to the lower thorax. This transforms the pyramidal infant thorax into the barrel-shaped one of adults 8 (Fig. 1‑3).


Sternum
The sternum is a flat bone that connects the ribs anteriorly via chondral tissue. The sternum consists of three regions: the manubrium, body, and xiphoid process (Fig. 1‑4). In the adult, it measures approximately 15 to 20 cm in length. The superior margin of the manubrium connects to the clavicles via the right and left clavicular notches at each corner. The sternoclavicular joints are diarthrotic synovial joints with an articular fibrocartilage disc in between (similar to the temporomandibular joint) (Fig. 1‑8). Each joint is covered by the anterior and posterior sternoclavicular ligaments. The sternocleidomastoid muscles attach to the superior margin of the sternum. The notch between the attachments of the sternocleidomastoid muscles is called suprasternal notch (Fig. 1‑4). Above the suprasternal notch, the interclavicular ligament connects the two clavicular heads. Laterally, the manubrium is attached to the first rib. The costal cartilage of the second rib is attached to the junction of the manubrium and body of the sternum (Fig. 1‑4). The sternothyroid and sternohyoid muscles attach to the posterior manubrium (Fig. 1‑8).
The anterolateral aspect of the body sternum is attached to the pectoralis major muscle. The superior and inferior sternopericardial ligaments attach to the posterior wall of the manubrium and xiphoid process, respectively (Fig. 1‑9). On either side of the posterior sternum, the transversus thoracis muscles take origin.
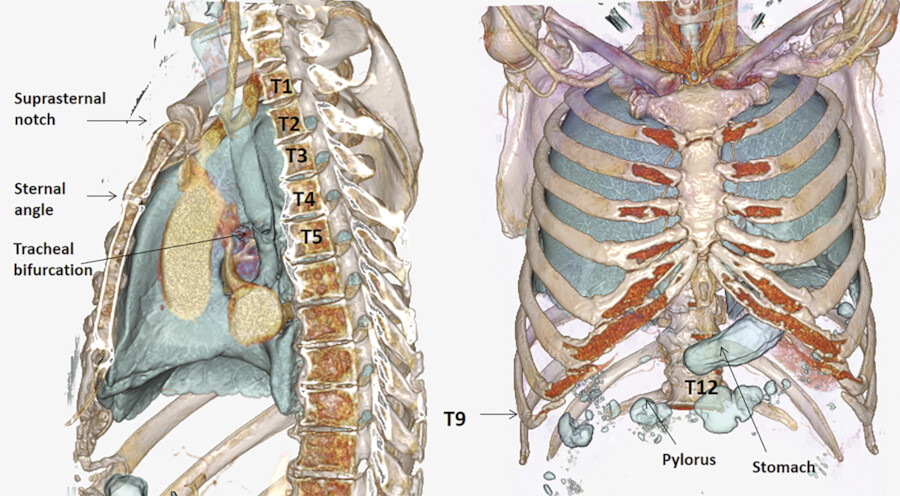
There are six notches on each side of the sternal body which receive the cartilages of the second through seventh ribs. The superior margin of the body forms a bony ridge which is called the sternal angle of Louis (Fig. 1‑4). This anatomical landmark corresponds with T3/T4 posteriorly (Fig. 1‑10). The tracheal bifurcation is usually located below the sternal angle. The joint between the manubrium and the body at the sternal angle allows the sternal body to move anteriorly. The xiphoid process varies in shape and length in different individuals. The seventh costal cartilages also articulate with the anterior or anterolateral portion of the xiphoid process.


The female adult sternum is located lower compared to the male sternum. 8 Compared to female, the body of the male sternum is usually twice as long as the manubrium. 9
The dominant blood supply to the sternum is provided by the internal mammary (thoracic) arteries that interconnect with the posterior intercostals, lateral thoracic, and transverse cervical arteries.
Anatomical Variations of the Bones
Minor variations of the anterior chest wall is common and can be seen in 30% of children and adults. 10 These variations include tilted sternum, prominent convexity of the anterior ribs and costal cartilages, mild pectus excavatum, and mild pectus carinatum (Fig. 1‑11).
There are various types of anomalies and deformities of the ribs. Common variants include developmental fusion of two or more ribs, articulation or bridge formation between two ribs, bifid rib (forked rib), and short rib. These morphological anomalies may have a sex predilection, and occur more frequently on the right side than on the left side. 3
In a bifid rib, the distal end of the rib appears bifurcated (Fig. 1‑12 a). The distal end may remain unfused or form a rounded hole or an elongated fissure. 11 The defect is filled with muscles which is supplied by a branch from the intercostal artery of the rib above it. The intercostal nerves may run on both sides of the rib defect. Bifid ribs are more common in males than females and occur most frequently in the third and fourth ribs. An intrathoracic rib is a rare type of bifid rib in which a supernumerary rib, arises from a rib or vertebral body 12 (Fig. 1‑12 b; Fig. 1‑13).
A cervical rib is a supernumerary or accessory rib arising from the seventh cervical vertebra on one or both sides. It may articulate to the first rib or end freely. It is seen in less than 1% of the population and is more common in females with slight predominance on the left side 13 (Fig. 1‑13). They are most commonly an incidental finding or are associated with the Klippel–Feil anomaly. The cervical is commonly associated with sacralization of the L5 lumbar spine. 14 The cervical rib can cause thoracic outlet syndrome by compression of the brachial plexus or subclavian artery between the cervical rib posteriorly, the anterior scalene anteriorly, and the first rib inferiorly. A lumbar rib is another anatomical variant manifested as a rudimentary or extra rib arising in the lumbar region. It is seen in roughly 1% of the population. 15 A lumbar rib is shorter than the 12th thoracic rib and its course tends to be more horizontal. Both cervical and lumbar ribs manifest an exaggerated development of the transverse process.
Eleven pairs of ribs occur in 5 to 8% of normal individuals and in one-third of patients with trisomy 21 syndrome. 16
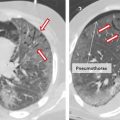
On frontal chest radiographs, it is common to see a thin, smooth, soft tissue density parallel the lower margins of the first and second ribs and the axillary portions of the lower ribs (Fig. 1‑14). These companion shadows represent the fat and muscles located in the intercostal spaces and should not be mistaken with pleural thickening or pneumothorax. The bony edge of the costal groove is seen as a thin, sharp hairline along the inferior margin of the ribs on frontal chest X-rays and should not be confused with a pneumothorax (Fig. 1‑14 a). Postoperative changes of the chest wall such as sternal wires, partial rib resection, and partial fusion of the ribs are common imaging findings.




Anatomical variation of the sternum is also common. If the fusion of the sternal bars is incomplete, a vertical fissure or perforation may be present in the sternum. The sternal foramen is a common asymptomatic developmental defect (Fig. 1‑2). It is probably due to incomplete fusion of the third and fourth ossification centers. The awareness of this anomaly is important in acupuncture practice. Cleft (bifid) sternum is a rare congenital defect due to failed midline fusion of the sternum. The cleft may be complete and incomplete. 17 Association with pectus excavatum, craniofacial hemangiomas, diastasis of the abdominal rectus muscles, and omphalocele is common. 18
Pectus Excavatum and Pectus Carinatum
Chest deformities are among the most common congenital anomalies. Pectus excavatum or funnel chest is the most common chest wall malformation occurring in approximately 1 out of every 500 live births (Fig. 1‑11). Pectus carinatum appears to be two to four times less frequent than pectus excavatum (Fig. 1‑15). The etiology is probably due to an imbalance growth of costal cartilage and ribs. 19 Both malformations can be present at birth but is usually recognized only during early childhood. Men are involved four times more often than women. 20
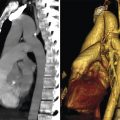
It is usually seen as an isolated congenital abnormality. However, it is occasionally associated with cardiac abnormalities, such as Marfan’s, Noonan’s, and Turner’s syndromes. 21 In pectus excavatum, there is a depression of the anterior chest wall as a result of dorsal deviation of the sternum and the third to seventh rib or costal cartilage. 21 There are characteristic findings on frontal chest radiography, including an indistinct border of the right side of the heart, left ward shift of the heart, and downward angulation of the anterior portions of the ribs. Computed tomography (CT) scan is the best technique to show the anomaly (Fig. 1‑16). Pulmonary or cardiac compression can result in restrictive lung disease and decreased right ventricle function (Fig. 1‑16).
Pectus carinatum presents by a protrusion of the sternum and ribs (Fig. 1‑16). In pectus carinatum, the lengths of costal cartilage are longer than usual so the ribs appear shorter. 19 The anomaly is usually asymptomatic and isolated but other diseases including scoliosis, Marfan’s syndrome, Morquio syndrome, or Poland’s anomaly may be found. Anomalously widened sternum with severe anterior angulation is rarely seen (Fig. 1‑17).



Chest Wall Pathologies
Plain radiographs are often used to evaluate chest wall pathologies. Cross-sectional techniques such as CT, sonography, and magnetic resonance imaging (MRI) have been shown to be more useful in the evaluation of muscle and soft tissue (Fig. 1‑18).
Rib asymmetry is an associated finding with scoliosis. Ribs on one side may be shorter. Most people with mild scoliosis demonstrate no rib asymmetry. 22
Chest wall pain after trauma can be due to a variety of factors, including osseous injuries such as fractures, injuries to the soft tissues such as muscle contusion or tears, and, less commonly, injury to the costal cartilage. Osseous injury involving the ribs and sternum is common. In a radiological assessment of the chest wall with CT scan attention to associated vascular and soft tissue injuries is of utmost importance. In fracture of the first and second ribs and the sternum attention to vascular injury is important. Fractures of the anterior ribs and even the sternum are common findings after vigorous cardiopulmonary resuscitation. Fracture of the left lower ribs may be associated with the spleen and left kidney injury and fractures of the rib necks can be a sign of spinal fracture.
The costal cartilage injury is best shown by MRI using fat-saturated T2-weighted imaging. 23 , 24 The most frequently injured site is reported at the first rib involving sternochondral or costochondral junctions. 23 Injury of the xiphoid process after trauma, cardiopulmonary resuscitation, or surgical incision can cause exuberant bony proliferation at this anatomical level.
Ribs and sternum are common sites of involvement in inflammatory diseases, primary tumors, or metastatic malignancies (Fig. 1‑18). Reactive periosteal thickening of the rib and sternum is common after trauma, surgery, and adjacent infectious processes. Rib or sternal osteomyelitis is relatively rare. Osteitis of the sternomanubrial joint is uncommon and could be related to rheumatoid arthritis, psoriatic arthritis, or ankylosing spondylitis (Fig. 1‑18). Fibrous dysplasia is a benign condition due to the proliferation of fibrous tissues in the bones. It is the most common cause of a benign expansile lesion of the ribs. 25 Imaging characteristics include, bone lucency with a “ground-glass” matrix, expansion, and remodeling. Lesions arising from chest soft tissue is also common (Fig. 1‑18).


Muscles of the Chest Wall
Functionally, the muscles of the chest wall are divided into two main groups: inspiratory and expiratory. 26 The principal muscle of inspiration is the diaphragm. This structure is reviewed in detail in Chapter 10, Diaphragm. With assistance from the external intercostal muscles, the diaphragm contracts during inspiration to enlarge the thoracic cavity. Other inspiratory muscles include the sternocleidomastoid and scalene muscles. These muscles are secondary accessory muscles that expand the chest volume by elevating the sternum and upper ribs of the thorax.
Major expiratory muscles include the rectus abdominal, internal oblique, and external oblique muscles. 1 These muscles decrease lung volumes by constricting the rib cage in a downward motion and by compressing the abdominal compartment and raising internal pressure.
However, these muscles only come into play as expiratory muscles during exercise or forced breathing maneuvers. At resting state, expiration is a passive process brought about by the recoil of the lungs and rib cage at the end of inspiration. The internal intercostal muscles also help in expiratory action moving ribs downward and inward.
Muscles of the Anterior Chest Wall
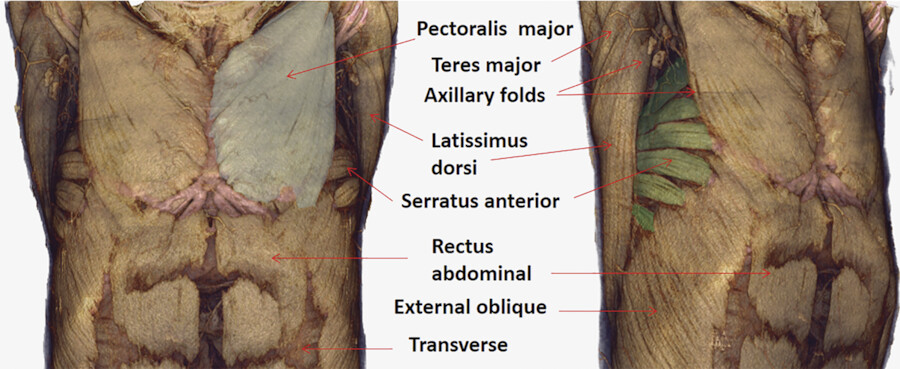
Major muscles of the anterior and anterolateral chest wall include the pectoralis major, pectoralis minor, serratus anterior, rectus abdominal, and external oblique (Fig. 1‑19 , Fig. 1‑20). The sternalis muscle is an uncommon accessory muscle (please see Fig. 1‑71 , Fig. 1‑72 at the end of the chapter).

Pectoralis Major
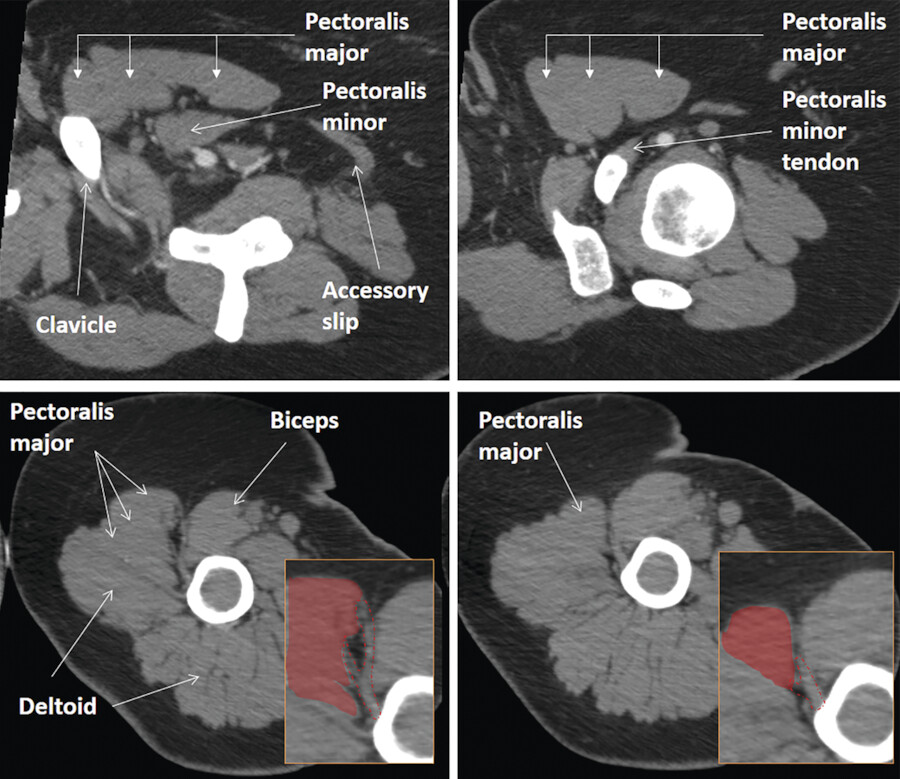
The pectoralis major is a fan-shaped muscle that covers the anterior superior portion of the chest and forms the anterior axillary fold. The pectoralis major has a complex morphology with two major segments. The proximal segment is subdivided into the clavicular and manubrial parts, and the distal segment into the sternocostal, costal and abdominal parts 28 , 29 (Fig. 1‑19 , Fig. 1‑20 , Fig. 1‑21 , Fig. 1‑22). The clavicular part arises from the medial half of the clavicle and the manubrial part from the manubrium and the medial aspect of the first and second ribs (Fig. 1‑21 b). The sternocostal part originates from the sternal body and medial aspect of the third to sixth ribs. The sternal origin of the muscle is from the lateral border of the sternum with an average width of 7 mm. 27 The middle part of sternum is not covered with muscle (Fig. 1‑20). The abdominal part is a separate layer that is located dorsal to the costal part, but occasionally originates from the aponeurosis of the external oblique abdominal muscle. The insertion tendon has a bilaminar U shape and attaches to the anterior surface of the humeral diaphysis, just lateral to the biceps brachii long head tendon (Fig. 1‑21 , Fig. 1‑22). 28 , 29 The clavicular and manubrial parts insert into the anterior limb of the U, the sternocostal part inserts into the inferior cup of the tendon, and the costal and abdominal parts insert into the posterior limb of the tendon. 28 This configuration of the pectoralis major muscle is analogous to the appearance of an unfolded handheld fan. 29
Each part of muscle has a distinct vascular and nerve supply that runs in the epimysium on the posterior surface of the pectoralis major muscle. 30 The muscle is supplied by the thoracoacromial artery (a branch of the axillary artery) and the lateral thoracic artery (a branch of the subclavian artery). It also receives segmental blood supply from the internal mammary artery by way of intercostal perforators. The pectoral muscles are innervated by the lateral and medial pectoral nerves, branches of the brachial plexus. The two pectoral nerves are usually connected immediately distal to the thoracoacromial artery by the ansa pectoralis. 31 The lateral branch innervates the upper parts and the medial branch innervates the lower parts of the pectoralis major. These nerves may be injured after trauma, breast surgery, lymph node dissection, and pectoralis major muscle transfers. Nerve injury causes muscle atrophy.
The main function of the pectoralis major is to adduct, internally rotate, and flex the humerus.
Rupture of pectoralis major muscle is uncommon. The muscle is at greatest risk when the shoulder is in an abducted, extended, and externally rotated position with maximal muscle tension. 32 Poland’s syndrome is a rare congenital anomaly characterized by the unilateral absence of the sternal portion of the pectoralis major muscle and sometimes ipsilateral symbrachydactyly (abnormally short and webbed fingers) 33 (Fig. 1‑23). It is more common in males and usually affects the right side. The pectoralis major muscle may be used either as a muscle or musculocutaneous flap for reconstructive chest wall surgery and subpectoral breast augmentation. 26


Pectoralis Minor
The pectoralis minor is a thin triangular muscle lying deep to the pectoralis major. It originates from the third, fourth, and fifth ribs near the costal cartilages (Fig. 1‑19 , Fig. 1‑21 , Fig. 1‑22).
However, the location of the costal origins of the muscle is highly variable. 34 Muscle fibers of the pectoralis minor ascend laterally to attach to the superomedial border of the coracoid process of the scapula (Fig. 1‑21 , Fig. 1‑22).
The axillary vessels and brachial plexus lie posterior to the muscle. The medial pectoral nerve supplies the pectoralis minor muscle. 31 The function of the pectoralis minor is to tilt the scapula anteriorly. Insertional tendinopathy of pectoralis minor is a cause of shoulder pain in weightlifters. 35
Pectoralis minimus is a small accessory muscle located under the pectoralis major muscle and medial to the pectoralis minor muscle. It originates from the first or second costal cartilages and inserts on the coracoid process. 36
Sternalis Muscle
The sternalis (parasternalis) muscle is an uncommon muscle variant of the anterior thoracic wall. 37 It lies between the superficial fascia and the pectoral fascia and runs parallel to the sternum. The size of the muscle is variable and ranges from a few short fibers to a well-formed muscle (Fig. 1‑24). It is found unilaterally (4.5–6%) or bilaterally (1.7%). 38 The muscle arises from the upper sternum and the infraclavicular region. The insertion point is variable including the pectoral fascia, lower ribs, costal cartilages, rectus abdominal muscle sheath, or the abdominal external oblique muscle aponeurosis. Innervation of the sternalis muscle is provided by branches of pectoral nerves (55%) and/or intercostal nerves (43%). 38 The function of the sternalis muscle still remains unknown, but it may help to elevate the lower chest wall. 39 On CT or MR studies, it is seen as a vertically oriented parasternal flat and bandlike structure surrounded by fatty tissue (Fig. 1‑24). When unilateral, it should not be confused with pathologies in mammogram or CT studies of the chest.

Serratus Anterior
The serratus anterior muscle arises from the lateral aspects of the first eight to nine ribs. The upper half of the muscle fibers attach to the superior angle and medial border of the scapula. The lower fibers attach to the medial aspect of the inferior scapular angle (please see Fig. 1‑71 , Fig. 1‑72 at the end of the chapter). The serratus anterior is frequently used to cover a lobar or mainstem bronchial stump. 40
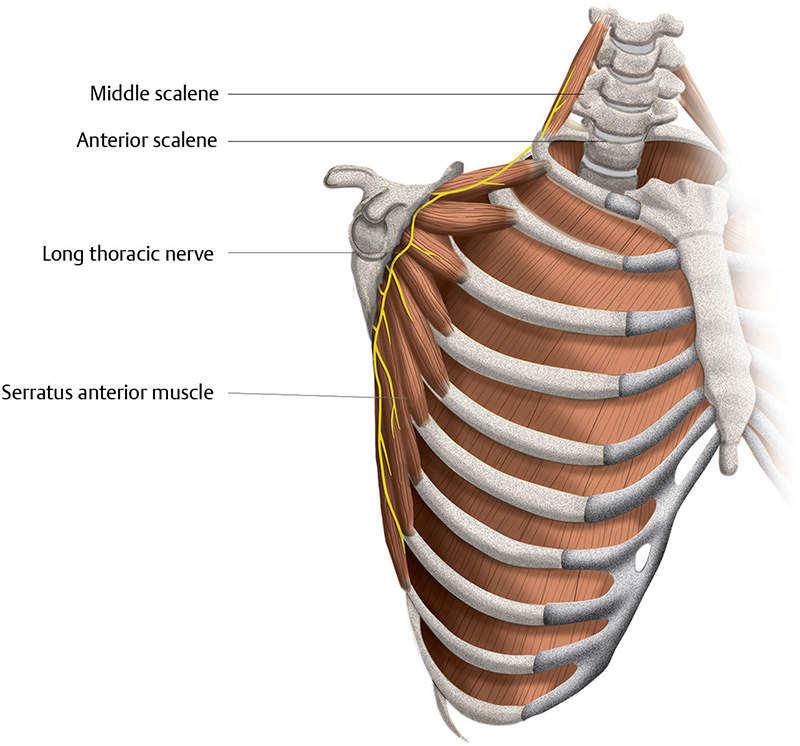
The serratus anterior muscle is supplied by the branches of the subscapular, thoracodorsal, and lateral thoracic arteries (Appendix image series). The thoracodorsal artery enters the muscle superior on its anterior surface and gives off multiple small branches before terminating in the latissimus dorsi muscle. 41 Innervation of the serratus anterior muscle is via the long thoracic nerve of Bell, which originates at the anterior rami of the C5 to C7 (or C8) spinal nerves. It travels inferiorly along the outer surface of the serratus anterior muscle entering the axilla (Fig. 1‑25). The long thoracic nerve can be visualized using high-resolution sonography. 42 The nerve may be injured during axillary lymph node dissection or radical mastectomy. The serratus anterior is important in shoulder stabilization during arm elevation, ensuring fixation, and upward rotation of the scapula. The classical clinical picture of nerve injury is scapular winging and the inability to elevate the arm. 43 Serratus anterior muscle pain syndrome is one of the causes of chronic chest pain of noncardiac origin. It is characterized by taut bands (tense muscle fibers), commonly described as trigger points. The trigger point can be treated by ultrasound-guided injection of anesthetic agents. 44 Elastofibroma is a relatively common pathology of the lateral chest that should not be mistaken with the serratus anterior muscle (Fig. 1‑26).

Abdominal Wall Muscles
Abdominal wall muscles cover part of the lower anterior and lateral chest wall. The rectus abdominal muscle originates from the xiphoid process and fifth to seventh costal cartilages and inserts on the pubic symphysis. Blood supply is provided by the superior and inferior deep epigastric arteries. The external oblique muscle originates from the inferior edge of the 6th through 12th ribs (Fig. 1‑27). The muscle fans out to insert on the iliac crest, linea alba, and pubic and inguinal ligaments. Innervation is from the inferior six intercostal nerves, and blood supply primarily derives from branches of the lower six posterior intercostal arteries. 45 The caudal part of the muscle is supplied by branches of the deep circumflex iliac artery. 46

The internal oblique muscle is located deep to the external oblique muscle. The very superior fibers insert into the inferior border of the last three to four ribs. The internal oblique muscle is vascularized by the ascending branch of the deep circumflex iliac artery, lower six posterior intercostal arteries, and lateral branches of the deep inferior epigastric artery. 47 The transverse abdominal muscle is the innermost muscle of the abdominal wall. It originates from the five lower ribs, thoracolumbar fascia, iliac crest, and the outer third of the inguinal. The muscle inserts medially into the rectus sheath though a broad aponeurosis.
Muscles of the Posterior Chest Wall
Muscles of the posterior chest wall include the latissimus dorsi, trapezius, serratus posterior superior, serratus posterior inferior, rhomboid, and erector spinae muscles.
Latissimus Dorsi
The latissimus dorsi is a large, flat, dorsolateral muscle on the trunk, which extends posterior to the arm. Medially, it is partly covered by the trapezius (Fig. 1‑28). The latissimus dorsi originates from the spinous processes of thoracic (T7–T12) vertebrae, inferior three or four ribs, inferior angle of scapula thoracolumbar fascia, and iliac crest. It wraps around the lateral chest wall to insert on the floor of intertubercular sulcus of the humerus (Fig. 1‑21). The latissimus dorsi and teres major muscles form the posterior axillary fold (Fig. 1‑19 , Fig. 1‑20 , Fig. 1‑21). Anterior and posterior muscle slips, found in 2% of cases, usually extend to pectoralis major or teres major 48 (Fig. 1‑21). Asymmetric muscle slip should not be confused with pathology (Fig. 1‑26).

The anterior and superior parts of the muscles along with the serratus anterior are supplied by the thoracodorsal artery, a branch of the subscapular circumflex artery. The posterior part is supplied by the intercostal perforators. Nerve supply is by the thoracodorsal nerve. 41 The latissimus dorsi is involved in extension, adduction against resistance, horizontal abduction, flexion from an extended position, and internal rotation of the shoulder joint. It also has a synergistic role in extension and lateral flexion of the lumbar spine. A tight latissimus dorsi may be one cause of chronic shoulder and back pain. The latissimus dorsi has been used for rotator cuff repair. It is the most frequently used muscle for the reconstruction of the lateral and anterior chest wall defects.
Rhomboid
The rhomboid minor and major muscles are posterior chest muscles that run obliquely between the medial margin of the scapula and spinal processes of T2 to T5 (Fig. 1‑28 , Fig. 1‑29). The rhomboid minor is located superior to the rhomboid major and both are covered by the trapezius muscle (please see Fig. 1‑71 , Fig. 1‑72 at the end of the chapter). Rhomboid muscles work along with the serratus anterior and pectoralis minor to maintain the scapula pressed against thoracic wall by retracting it toward the spine. The arterial supply is provided by the dorsal (descending) scapular artery. This artery also supplies the levator scapulae and trapezius muscles. The dorsal scapular artery is the deep branch of the transverse cervical artery (a branch of the thyrocervical trunk).

The rhomboids are innervated by rhomboid nerve which is the terminal branch of dorsal scapular nerve. The dorsal scapular nerve is single nerve that arises from the C5 spinal nerve and occasionally from the C3, C4, and C6 roots. 48 , 49 It penetrates the middle scalene muscle, and runs on the ventral side of the levator scapulae muscle and rhomboid muscles near the medial border of the scapula. Paralysis of the suprascapular nerve commonly occurs in avulsion injuries of the brachial plexus causing disturbance of the elbow flexion and shoulder elevation. Transfer of the spinal accessory nerve to the suprascapular nerve is performed most often to treat the problem. 50
Trapezius
The trapezius is a large muscle that covers the posterior aspect of the occipital region of the skull, the neck, and the superior part of the thorax and attaches the upper limb to the skull and vertebrae (Fig. 1‑28). The trapezius muscle fibers are divided into superior, middle, and inferior fibers, each of which exhibits a different action. The superior fibers originate at the superior nuchal line and external occipital protuberance and reach the lateral portion of the clavicle. The middle fibers originate from the spinous processes of the seventh cervical to the third thoracic vertebrae and are inserted on the acromion. This part represents the strongest portion of the muscle that helps to retract the scapula. The inferior fibers arise in most thoracic spinous processes and are inserted along the spine of the scapula. The inferior part depresses the scapula and lowers the shoulder.
Its major blood supply is the transverse cervical artery, a branch of the thyrocervical trunk.
Its secondary blood supply includes occipital branches and intercostal perforators.
The accessory nerve (11th cranial nerve) provides motor supply to the superior and middle parts of the trapezius and also to the sternocleidomastoid muscles. 50 , 51 Damage of the accessory nerve results in trapezius muscle weakness, atrophy, and shoulder disability. The inferior portion of the muscle is innervated by the C3 and C4 cervical plexus. During modified radical neck dissection, the main identification point of the accessory nerve is in the posterior triangle, behind the posterior margin of the sternocleidomastoid muscle at Erb’s point, where the greater auricular nerve crosses the accessory nerve. 52 The knowledge of anatomical variations of the accessory nerve is of clinical importance during neck dissection. Lee et al studied the anatomy of the accessory nerve at level IIb. 53 They found that the nerve passes anterior to the internal jugular vein in 40% and posterior to the vein in 57% of the cases. 53
Myofascial pain syndrome is a common cause of chronic musculoskeletal pain. This syndrome presents clinically as referred pain, a limited range of joint motion, and a local twitch response following mechanical stimulation of certain muscular and fascial areas, also known as myofascial trigger points. 54 Myofascial trigger points are identified by palpation of a locally painful knot during clinical examination. Active trigger points frequently originate in the trapezius muscle.
Serratus Posterior Superior Muscle
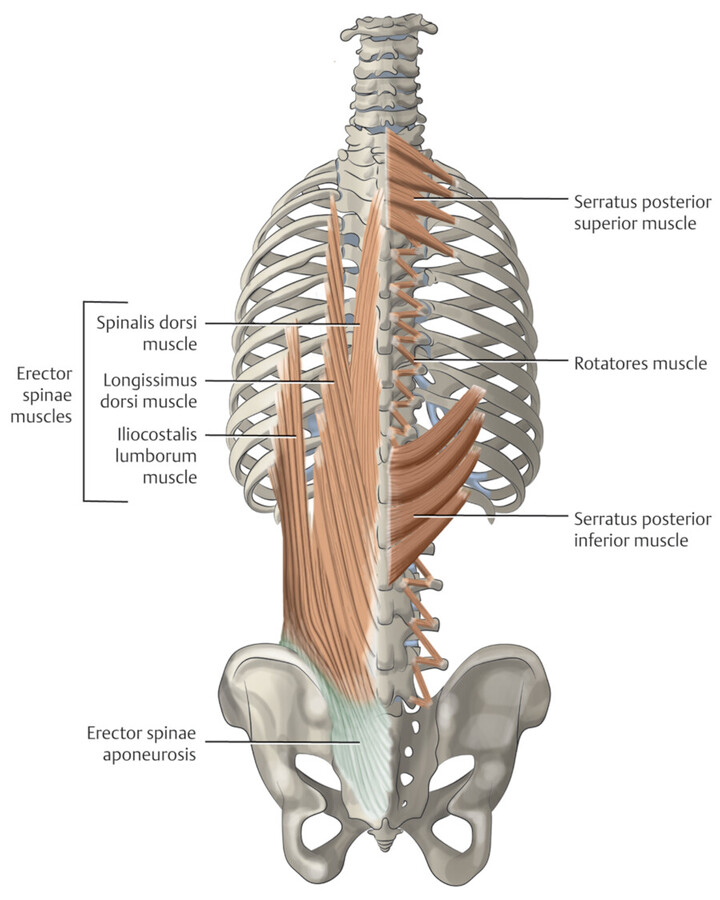
The serratus posterior superior is a small deeply located muscle covering a small portion of the posterosuperior chest wall (Fig. 1‑30 , Fig. 1‑31). It covers the erector spinae muscles and is overlaid by the rhomboid muscles (please see Fig. 1‑71 , Fig. 1‑72 at the end of the chapter). The muscle extends between the spinous processes of the C7 to T3 and the upper borders of the second through fifth posterior ribs. The serratus muscles are supplied by the intercostal arteries and innervated by the intercostal nerves. The serratus posterior superior elevates upper ribs to help deep inspiration.

Serratus Posterior Inferior Muscle
The serratus posterior inferior muscle is also a relatively small, comb-like muscle covering a small portion of the posterosuperior abdominal wall and the posteroinferior chest wall (please see Fig. 1‑71 , Fig. 1‑72 at the end of the chapter). It covers the erector spinae muscles and overlaid by the latissimus dorsi muscle. The serratus posterior inferior extends from the spinous processes of T11 to L2 to insert onto the lower border of the last four ribs lateral to the iliocostalis muscle insertions (Fig. 1‑30 , Fig. 1‑31). Medially, its aponeurosis blends with the thoracolumbar fascia. The serratus posterior inferior muscle contributes to forced expiration and extension/rotation of the trunk.
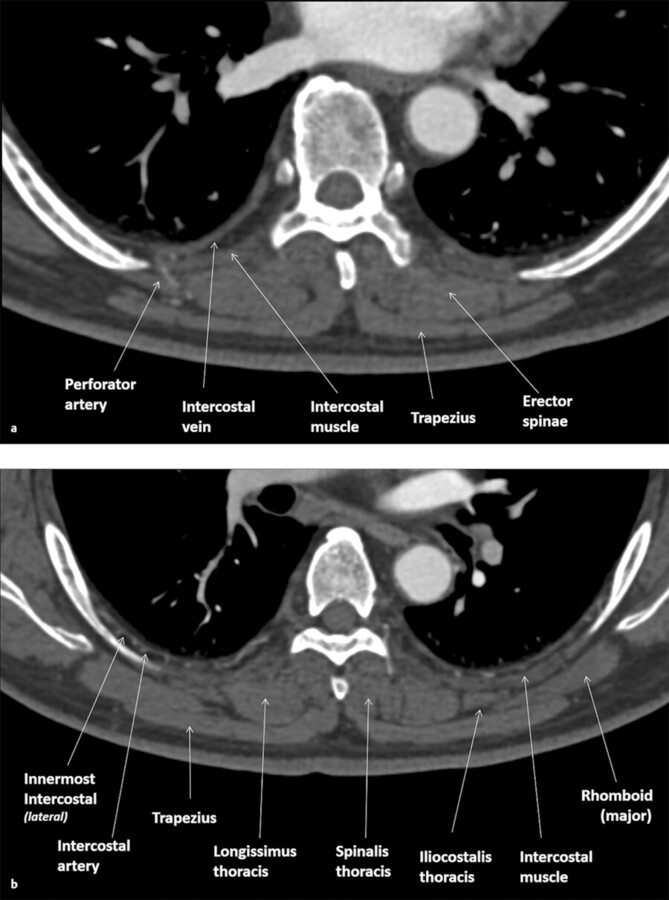
Erector Spinae Muscles
The erector spinae are a deep muscle group that runs parallel to the spine and covers the posterior medial walls of the chest and abdomen. It is divided into three columns by three muscles. These muscles from lateral to medial include the iliocostalis, longissimus, and spinalis (Fig. 1‑30 , Fig. 1‑31). Each muscle is also subdivided into three parts depending on the anatomical coverage. For example, the iliocostalis is partitioned into the lumborum, thoracis, and cervicis. The longissimus and spinalis are partitioned into the thoracis, cervicis, and capitis.
The iliocostalis attaches to the transverse process of C6–C4 at its cervical levels. At the thoracic level, it interconnects the posterior ribs lateral to the rib angles (please see Fig. 1‑71 , Fig. 1‑72 at the end of the chapter). The longissimus is located between the other two muscles and becomes larger in the lower thoracic and lumbar regions. It mainly originates from the transverse processes and posteromedial ribs and interconnects them together. At its uppermost end, the longissimus connects to the mastoid process of the temporal bone. The spinalis muscle is the smaller one on the sides of the spinous processes and connects them together.
Thoracolumbar Fascia
The thoracolumbar fascia is a complex of several membranous layers that separates the paraspinal muscles from the muscles of the posterior abdominal wall, quadratus lumborum, and psoas major (please see Fig. 1‑71 , Fig. 1‑72 at the end of the chapter). This complex structure wraps around the erector spinae muscles of the lower back and sacral region (Fig. 1‑31).
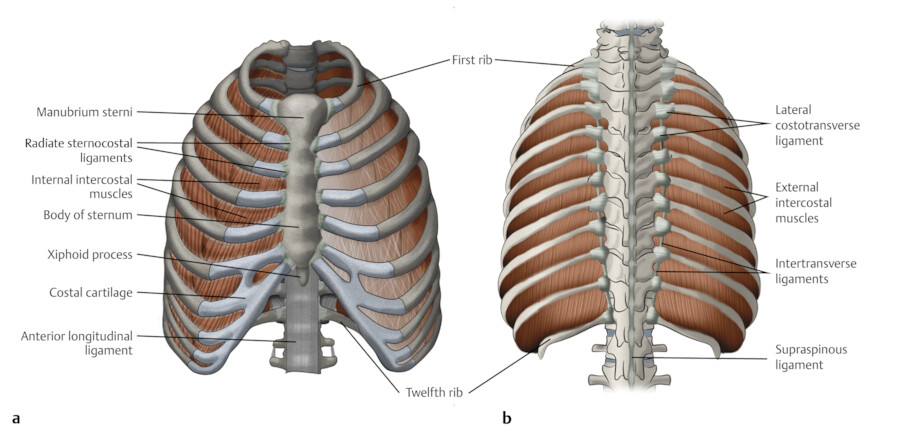
Intercostal Muscles
The intercostal muscles include the external, internal, and innermost muscles 5 (Fig. 1‑32 , Fig. 1‑33 , Fig. 1‑34). The external intercostal muscles form the outer layer of the intercostal muscles extending between the costochondral junction to the tubercle of the rib. They are thicker than the internal intercostal muscles. The internal intercostal muscles form the inner layer of the intercostal muscles extending between the sternocostal junction to the tubercle of the rib. The fibers of external intercostal are oriented obliquely from a more posterior point on the upper rib to a more anterior point on the lower rib. The fibers of internal intercostal are oriented obliquely in an opposite direction, from a relatively anterior point on the upper rib to a more posterior point on the lower rib 4 (Fig. 1‑32 , Fig. 1‑33 , Fig. 1‑34 , Fig. 1‑35).
In the parasternal region, the external intercostal muscle is replaced by the anterior intercostal membrane, a thin aponeurosis (Fig. 1‑35). The only muscle fibers in the parasternal region are those of the internal intercostals also known as parasternal intercostals (Fig. 1‑35, Fig. 1‑36). In the paravertebral region, the internal intercostal muscle may be absent. Instead, the space is covered by the levatores costarum muscles and the posterior intercostal membrane (Fig. 1‑37). The 12 levatores costae are small muscles extending between the tip of the transverse process of the vertebra and the inferior rib on each side (Fig. 1‑30). In each intercostal space, thin but firm layers of fascia cover the outer surface of the external intercostal.
The innermost intercostal muscles are variable, incomplete, and deepest muscle layer. Depending on location, these muscles are divided into three groups: subcostalis, lateral innermost, and transversus thoracis. The subcostalis muscles are located posterolaterally and extend over two or three ribs (Fig. 1‑14 , Fig. 1‑37). They are better developed in the lower chest wall (please see Fig. 1‑71 , Fig. 1‑72 at the end of the chapter). The lateral group fibers run parallel to the fibers of the internal intercostal muscles but separated from each other by intercostal nerves and vessels. The parasternal intercostal regions are covered on their inner surface by four to five thin muscle slips known as the transversus thoracis (triangularis sterni, or sternocostalis). The transversus thoracis originates from posterior surface of the lower sternal body and the xiphoid process. Its muscle fibers run laterally and superiorly (parallel to the anterior external intercostal fibers) to insert on the second through sixth ribs/costal cartilages (Fig. 1‑34). The most frequent lowest rib attachment is the sixth rib. 55 The highest muscle attachment may reach to the second rib to cover the internal thoracic artery. Variants including complete absence, asymmetry, presence of a slip attached from the second to fourth rib cartilages and continuation with the fibers of the transverse abdominal muscle have been described.
All the intercostal muscles are innervated by the intercostal nerves and supplied by the intercostals arteries. The main intercostal nerve runs between the pleura and the inferior aspect of the rib and gives off the external and internal branches to the corresponding intercostals muscles. The intercostal nerve also gives off branches to the transversus thoracis and several abdominal muscles.
The primary effect of the intercostal muscle contraction is to displace the ribs. 56 Ribs have limited motion at the vertebral end. The costovertebral and costotransverse joints together form a hinge. Therefore, the respiratory movements of the rib occur primarily through a rotation around the long axis of its neck. With each inspiration, the ribs are moved in the cranial direction, and the sternum will be displaced anteriorly. Consequently, both the lateral and anteroposterior diameters of the rib cage increase with inspiration. This implies that the muscles that elevate the ribs have an inspiratory effect on the rib cage, whereas the muscles that lower the ribs have an expiratory effect on the rib cage (Fig. 1‑38). The inspiratory effect of the intercostal muscle function is primarily related to the contraction of the upper posterior external intercostal muscles and to a lesser degree to the levatores costae and the parasternal intercostal muscles. The lower internal interosseous intercostal and transversus thoracis muscles have an expiratory mechanical advantage. 57 Spontaneous quiet expiration in supine humans is essentially a passive process.




Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


