CASE 116 A teenage boy presents with recurrent upper abdominal pain for several days after beginning a new exercise routine. Fig. 116.1 (A,B) Contrast-enhanced axial CT images demonstrate a well-circumscribed fatty lesion anterior to the stomach (arrows). The lesion shows central fat density with internal wisps of soft tissue density and surrounding inflammatory soft tissue stranding. Contrast-enhanced axial computed tomography (CT) images demonstrate a well-circumscribed fatty lesion anterior to the stomach. The lesion shows central fat density with internal wisps of soft tissue density and surrounding inflammatory soft tissue stranding. The absence of adjacent gastric wall thickening is a pertinent negative finding (Fig. 116.1). Focal omental infarction The greater omentum, which is composed of a double layer of peritoneum, originates from the greater curvature of the stomach and extends anteroinferiorly to drape over the transverse colon. It has a variable length of 15 to 36 cm. “Omental infarct” actually represents only a segmental infarction of the greater omentum; infarction of the entire omentum has not been reported. Following an insult, the classic pathologic findings of infarction develop, including vascular congestion or thrombosis, tissue necrosis, inflammatory cell aggregation, and hemorrhage. The majority of omental infarction occurs in the right aspect of the omentum.
Clinical Presentation
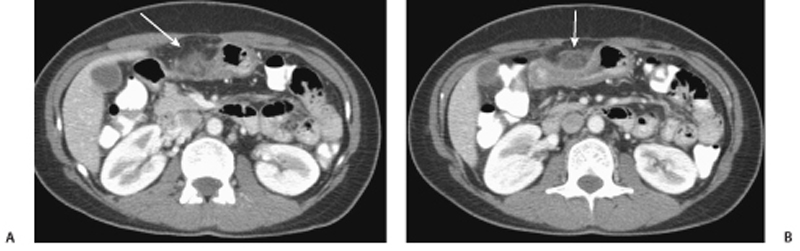
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Clinical Findings
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


