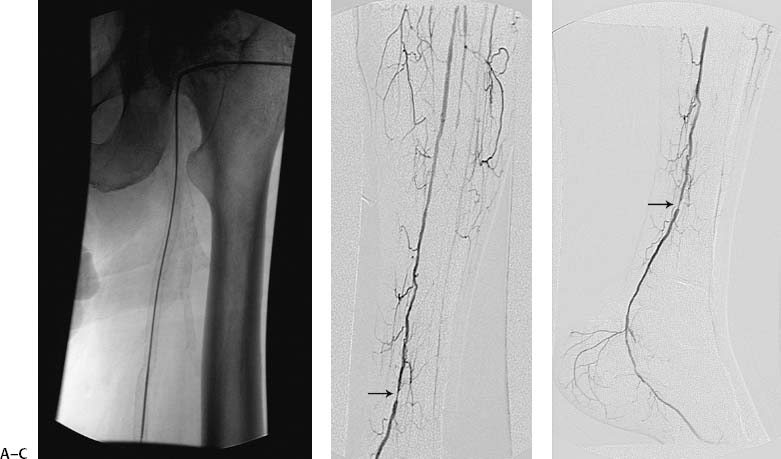
CASE 12 A 58-year-old male with extensive history of coronary artery disease presented with a nonhealing foot ulcer. Doppler exam revealed very weak pulse signals in the crural arteries. Ankle-brachial index was 0.2. Figure 12-1 Posterior tibial artery angioplasty. (A) Fluoroscopic image shows antegrade access into the common femoral artery. (B) Anterior and (C) lateral views of digital subtraction angiogram show distal stenosis of the posterior tibial artery (small arrows). (D) Fluoroscopic image shows guidewire in the posterior tibial artery. (E) Fluoroscopic image shows balloon angioplasty of stenosis. (F) Final digital subtraction angiogram shows alleviation of the stenosis. The right common femoral artery was catheterized using the Seldinger technique, and a 5-French (F) sheath was placed. A pigtail catheter was advanced into the abdominal aorta, and aortography with bilateral runoff was performed. The contralateral common femoral artery was then catheterized over the aortic bifurcation. A lower extremity angiogram was performed revealing complete occlusion of the anterior tibial and peroneal arteries and a high-grade stenosis of the left posterior tibial artery at the level of the distal calf. High-grade stenosis of the posterior tibial artery with associated nonhealing foot ulcer. The right common femoral artery had already been catheterized for arteriography. An antegrade puncture into the left common femoral artery was performed, and a 5F sheath was inserted (Fig. 12-1A). Five thousand units of heparin were administered intra-arterially. Lower leg arteriography was then performed to define the lesion (Fig. 12-1B, C). An endhole catheter was advanced down the superficial femoral artery, and a 0.018-inch guidewire was used to cross the stenosis (Fig. 12-1D). The end-hole catheter was then exchanged for a 3 mm- × 2 cm-long low-profile 0.018-inch angioplasty balloon catheter, which was used to dilate the lesion (Fig. 12-1E). Follow-up arteriography showed no residual stenosis with rapid antegrade flow to the foot (Fig. 12-1F). Revascularization enabled the foot ulcer to heal in subsequent weeks.
Clinical Presentation

Radiologic Studies
Angiogram
Diagnosis
Treatment
Infrapopliteal Angioplasty
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


