12 Malignant Obstructive Jaundice
Christopher R. Bailey and Kelvin Hong
12.1 Introduction
Malignant tumors cause approximately 70 to 90% of all biliary obstructions. Several types of malignancies can lead to bile outflow obstruction from the liver to the intestinal tract, including pancreatic adenocarcinoma, cholangiocarcinoma, and metastatic disease. 1 , 2 Although biliary obstruction primarily occurs in advanced disease, it is often the initial presenting sign of malignancy. As such, many of these cancers remain undiagnosed until the later stages of the disease.
Malignant biliary obstruction typically presents as painless jaundice (yellowing of the skin, sclera, and mucous membranes) and dark urine secondary to hyperbilirubinemia. 2 , 3 Patients with obstructive jaundice also complain of pruritus and are at risk of developing life-threatening biliary infections, including cholangitis, because of persistent biliary stasis. Interventions that restore biliary flow through stenting or external drainage can decrease serum bilirubin levels and improve quality of life through symptomatic relief 2 (▶ Fig. 12.1). In addition, these interventions may allow for further medical and surgical therapies to treat the patient′s underlying malignancy. 3

The management of these complex and debilitating conditions requires a multidisciplinary medical, surgical, and interventional approach. Interventional radiologists and gastroenterologists use diagnostic imaging and image-guided percutaneous and endoscopic methods for both treatment and symptomatic palliation. 4 In the discussion that follows, we review preprocedural imaging and evaluation, indications for percutaneous intervention, specific interventional and endoscopic techniques, and treatments for malignant obstructive jaundice.
12.2 Patient Evaluation and Preprocedural Imaging
It is important to take into account the patient′s baseline liver function and overall functional status before any procedure is performed. 2 Although percutaneous and endoscopic interventions are minimally invasive, patients with significant hepatic dysfunction may not have the functional reserve to overcome even minimal complications. 5 Baseline renal function must also be taken into account as iodinated contrast is often needed to opacify the biliary system and surrounding vascular structures. In addition, patients with gastrointestinal and neuroendocrine cancers affecting biliary drainage often have significant coagulopathies that may also alter the risk/benefit ratio for a particular intervention. Finally, the clinician must also obtain baseline imaging of the biliary system and surrounding extrahepatic structures.
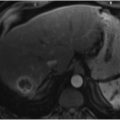
Cross-sectional imaging with multidetector computed tomography (MDCT) and magnetic resonance imaging (MRI) is useful when evaluating a patient with malignant obstructive jaundice before interventions are performed. CT allows for reformatting of images in multiple planes with 3D (three-dimensional) reconstruction to better define metastatic spread, including lymph node and vascular involvement and the type/degree of biliary obstruction. 2 , 4 , 6 MRI, specifically MR cholangiopancreatography (MRCP), also allows for multiplanar evaluation of the biliary system and surrounding organs (▶ Fig. 12.2). MRCP has a high sensitivity for the detection and localization of biliary obstruction (96–99%) but lower specificity with respect to differentiating between benign and malignant causes (85%). 7 , 8 The major disadvantage of MRCP is the length of time required for image acquisition, but this is accompanied by the benefit of greater image resolution and freedom from ionizing radiation. Finally, evaluation with ultrasound (US) allows for point-of-care evaluation of biliary ductal dilation and stone disease and identification of vascular structures. However, patient positioning, body habitus, and the presence of surrounding extrahepatic structures can limit US evaluation; additionally, US imaging is an operator-dependent modality. 6

12.3 Diagnostic Endoscopic Evaluation
12.3.1 Endoscopic Retrograde Cholangiopancreatography
Patients with biliary obstruction usually undergo initial evaluation with endoscopic retrograde cholangiopancreatography (ERCP). ERCP is an outpatient procedure that combines gastrointestinal endoscopy with fluoroscopy to evaluate the pancreatic and bile ducts. With the patient under procedural sedation or general anesthesia, an endoscope is inserted into the oral pharynx and is advanced into the second part of the duodenum to the level of the ampulla of Vater, an anatomic landmark where the common bile duct (CBD) and pancreatic duct join and enter the duodenum. The ampulla is cannulated and contrast is injected into the confluence to opacify the CBD, pancreatic duct, and proximal bile ducts. 9 After identification of a biliary stricture, ERCP is used to obtain brush cytology or biliary biopsy, if the obstruction is more distal (closer to the ampulla of Vater). The sensitivity of brush cytology is poor for diagnosing a malignant cause of stricture (23–56%); however, the specificity is quite high (95%). 7 , 9 The sensitivity is improved to 70% when brush cytology is combined with endobiliary biopsy with high specificity (100%). 7 Because ERCP allows for access to the intrahepatic and extrahepatic bile ducts through natural orifices, patients with contraindications to percutaneous methods such as significant coagulopathies, ascites, and polycystic liver disease can be safely evaluated with this technique. 6
The most common complication is post-ERCP pancreatitis, which can occur in up to 5 to 7% of all procedures and is usually mild and self-limited. 10 Other risks include intestinal perforation from endoscopic insertion and bleeding from the sphincterotomy. The decision to pursue ERCP should be made carefully. If therapeutic interventions are unlikely to be performed, most academic centers opt for noninvasive imaging methods such as MRCP to investigate biliary obstruction and determine whether it is secondary to a benign or malignant process. 8 , 11 Although cannulation of the ampulla of Vater is successful in approximately 85 to 98% of procedures, this technique is operator dependent and can be quite difficult to perform in patients with surgically altered anatomy. 12
12.3.2 Endoscopic Ultrasound
Endoscopic US (EUS) employs a technique similar to that of ERCP to evaluate causes of biliary obstruction. First, an endoscope with a US probe and biopsy needle is inserted through the mouth. The scope is advanced through the gastrointestinal tract to the level of the culprit lesion. The needle is deployed from the endoscope into the mass/stricture under US guidance and a fine needle aspirate (FNA) is obtained. For diagnosing malignancy, EUS has an overall sensitivity of 43 to 86%, with better sensitivity for more distal lesions. 7 , 13 The complications associated with EUS-FNA are similar to those seen with ERCP. The rates of pancreatitis associated with EUS-FNA through pancreatic tissue have been reported to be approximately 2%. 14 As with any endoscopic procedure, there is a risk of intestinal perforation. 7 Infection and hemorrhage have also been reported after EUS, but the incidence of these complications is low. Finally, there is a theoretical risk of malignant seeding with EUS given that the needle is advanced into malignant tissues and retracted back into the gastrointestinal tract. 7 , 15
12.3.3 Intraductal Ultrasound
Intraductal US (IDUS) is a relatively new technology that is used in combination with ERCP. IDUS allows for US evaluation directly within a bile duct. The sensitivity of IDUS for identifying malignant lesions ranges from 80 to 90% with a specificity of 83%. 7 IDUS does not itself provide tissue diagnosis but does allow for limited staging using a set of established imaging criteria for determining whether a lesion is benign or malignant. 16 , 17 The potential complications of IDUS are similar to those of ERCP and EUS, given the endoscopic approach and required cannulation of the CBD or pancreatic duct.
12.3.4 Peroral Cholangioscopy
Peroral cholangioscopy (POC) allows for direct visualization of the bile ducts and evaluation of stone disease with the use of an optical probe. Cholangioscopy is usually performed after noninvasive imaging and ERCP with diagnostic brushing have failed to provide a diagnosis. 18 A series of diagnostic criteria has been established to determine whether a biliary stricture is malignant or benign. The most sensitive and specific sign for malignancy is the visualization of dilated and tortuous blood vessels. 7 With regard to tissue diagnosis, POC with forceps biopsy has demonstrated a diagnostic accuracy ranging from 49 to 82% when used to evaluate indeterminate biliary lesions. 7 , 19 , 20 Cholangitis is the most common complication reported with POC, occurring in up to 14% of procedures. 7 Other complications associated with cannulation of the bile ducts and endoscopy may include pancreatitis and bowel perforation. 18
12.4 Diagnostic Percutaneous Evaluation
12.4.1 Percutaneous Transhepatic Cholangiography
Percutaneous transhepatic cholangiography (PTC) is reserved for situations in which less invasive methods such as MRCP and ERCP are unable to fully opacify the biliary system and identify the area of obstruction. PTC is also helpful in patients with surgically altered anatomy, when cannulation of the bile ducts with ERCP is difficult. 6 PTC allows for delineation of the intrahepatic and extrahepatic biliary tree, characterization of lesions, and identification of any bile leaks. As mentioned earlier, PTC is contraindicated in patients with significant ascites, severe coagulopathies, or polycystic liver disease. In addition to being used to evaluate the biliary system, PTC is performed as the first step before percutaneous biliary drainage (PBD) and percutaneous transhepatic biliary stenting are attempted.
After an appropriate preprocedural evaluation has been carried out (as described earlier), the patient is placed in a supine position and is administered procedural sedation or general anesthesia. After sterile preparation and draping are performed, the skin is anesthetized inferior to the costophrenic angle but superior to the hepatic flexure of the colon. 6 , 21 Under US guidance, a 22-guage Chiba needle (Cook Inc., Bloomington, IN) is inserted at approximately the mid-axillary line into one of the peripheral ducts. Once the interventional radiologist is satisfied with positioning of the needle, the inner stylet is removed to check for bile reflux and/or to inject a mixture of 1:1 water-soluble contrast to confirm positioning within a peripheral duct. Once contrast is seen flowing away from the entry point opacifying the biliary system, a cholangiogram can be performed to thoroughly examine the biliary tree and identify obstructions. 6 , 22 If an obstruction is identified, PBD can be performed for palliation, preoperative staging and decompression, or diversion of bile away from an identified bile leak (▶ Fig. 12.3) and can be utilized for unilateral or bilateral lobe drainage (▶ Fig. 12.4). In addition, endobiliary biopsy can be performed at the time of PTC as a secondary method for obtaining a tissue diagnosis.


Related posts:
 9 Interventional Management of Benign Refractory Ascites
9 Interventional Management of Benign Refractory Ascites
 13 Acute Cholecystitis, Cholelithiasis, and Choledocholithiasis
13 Acute Cholecystitis, Cholelithiasis, and Choledocholithiasis
 15 Hepatocellular Carcinoma: Staging and Clinical Management
15 Hepatocellular Carcinoma: Staging and Clinical Management
 23 Yttrium-90 Radioembolization of Malignant Liver Tumors
23 Yttrium-90 Radioembolization of Malignant Liver Tumors
 27 Image-Guided Colorectal Obstruction Management
27 Image-Guided Colorectal Obstruction Management
 28 Obesity and Bariatric Embolization
28 Obesity and Bariatric Embolization
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


