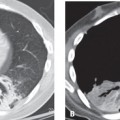
CASE 123 63-year-old man with Sjögren syndrome and abnormal chest radiography (not illustrated) Unenhanced chest CT (Figs. 123.1A, 123.1B, 123.1C, 123.1D, 123.1E, 123.1F) demonstrates a combination of variable-size thin-walled cysts, bulla, and nodules throughout both lungs. Some nodules are well defined whereas others are irregular. Several nodules contain eccentric calcifications (arrows) and others abut the cystic lesions (arrowhead). Nodular Parenchymal Amyloidosis with Lymphoid Interstitial Pneumonia (LIP) • Granulomatous Disease • Metastatic Lung Cancer • Rheumatoid Nodules Amyloidosis is a generic term that describes a group of disorders characterized by extracellular deposition of abnormal insoluble protein and protein derivatives that show apple green birefringence when stained with Congo red and viewed with polarized light. There are two distinct classes based on the type of amyloid deposited. Primary amyloid light (AL) chain disease is characterized by extracellular deposition of immunoglobulin light chains produced by plasma cells (i.e., plasma cell dyscrasia) and is responsible for most clinically significant cases with respiratory disease. Secondary amyloid A (AA) chain disease is most commonly seen in association with rheumatoid arthritis, but is also associated with other chronic inflammatory disorders (e.g., inflammatory bowl disease, chronic systemic inflammatory disorders, and chronic pulmonary infections) as well as Sjögren syndrome and lymphoid interstitial pneumonia (LIP) (see Case 109). Amyloidosis may be defined by anatomical extent as either localized (20%) or systemic (80%). Localized amyloidosis results from focal deposition of AL proteins and usually causes symptoms. Systemic amyloidosis results from deposition of AL proteins in multiple organ systems, including the lungs. In these latter cases, amyloid deposition is an incidental finding that only rarely causes symptoms. Respiratory system involvement occurs only with primary and not secondary amyloidosis. Thoracic amyloidosis most often manifests with cardiac involvement (restrictive cardiomyopathy). Involvement in order of frequency then includes the airway s (i.e., tracheobronchial tree) (see Case 22), the lung parenchyma (solitary or multiple nodules), the interstitium (diffuse alveolar septal thickening), and the mediastinal and hilar lymph nodes
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
![]()
Stay updated, free articles. Join our Telegram channel




Full access? Get Clinical Tree


