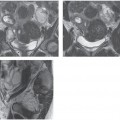
CASE 131 A 34-year-old woman presents with severe pelvic pain and a history of dysmenorrhea. Fig. 131.1 (A,B) Sagittal and coronal MR T2-weighted images demonstrate a large, heterogeneous, low signal intensity myometrial mass (arrow) displacing the endometrial stripe, most consistent with a uterine leiomyoma. (C) The lesion shows homogeneous early enhancement on a sagittal MR image obtained after the intravenous administration of gadolinium. Sagittal and coronal magnetic resonance (MR) T2-weighted images (Fig. 131.1A,B) demonstrate a large, heterogeneous fundal mass displacing the endometrial stripe, most consistent with a uterine leiomyoma. The lesion shows homogeneous early enhancement on a sagittal MR image obtained after the intravenous (IV) administration of gadolinium (Fig. 131.1C). Leiomyoma Uterine leiomyomas, also called fibroids or myomas, represent the most common gynecologic tumor, occurring in ˜20 to 30% of women in their 2nd to 3rd decades. They arise from smooth muscle cells of the myometrium and contain variable amounts of fibrous tissue; some of these lesions have a high rate of growth resulting in different types of degeneration, such as hyaline, myxoid, and hemorrhagic (red) degeneration. These histopathologic features are responsible for the variable appearance of leiomyomas at imaging but are unrelated to clinical symptoms. The location of these lesions within the uterus deeply affects clinical presentation; according to their location within the uterus, leiomyomas are classified as submucosal, intramural, or subserosal. Submucosal leiomyomas are the least common (only 5%) but the most commonly symptomatic, causing dysmenorrhea, menorrhagia, and infertility. Intramural and subserosal leiomyomas are usually asymptomatic, but they may be associated with menorrhagia and menstrual irregularities; moreover, some subserosal leiomyomas may become pedunculated and grow laterally within the folds of broad ligament (intraligamentous leiomyomas), resembling ovarian masses at imaging. Uterine leiomyomas may also have unusual patterns of growth and extent outside the uterus, as seen in parasitic leiomyomas (which incorporate an extrauterine blood supply and can become separated from the uterus), IV leiomyomatosis, intraperitoneal leiomyomatosis, and benign metastatic leiomyomas. Clinical presentation varies according to the size, location, and number of leiomyomas. Patients commonly present pelvic pain (usually during menstruation), menorrhagia (chronic loss of blood may cause severe anemia), and infertility. Other symptoms include urinary frequency and urgency resulting from pressure on the bladder or constipation and difficult defecation from pressure on the colon.
Clinical Presentation
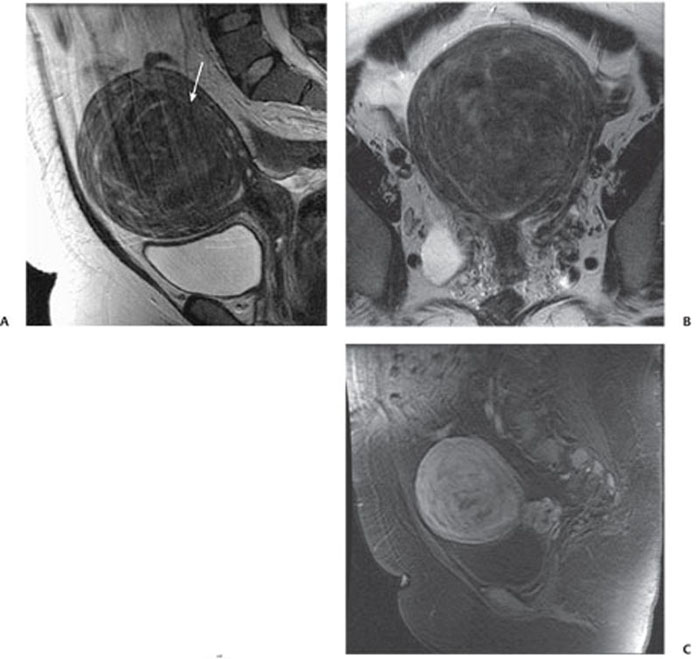
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Clinical Findings
Complications
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


