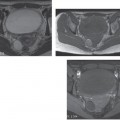
CASE 132 A 32-year-old woman presents with abdominal tenderness and fever. Fig. 132.1 (A,B) Contrast-enhanced axial CT images of the pelvis demonstrate a heterogeneously enhancing area associated with mild fat stranding in the left adnexal region with an associated oval-shaped fluid density structure (arrow). There is free fluid in the pelvis. Contrast-enhanced axial computed tomography (CT) images of the pelvis (Fig. 132.1) demonstrate a heterogeneously enhancing area associated with mild fat stranding in the left adnexal region with an associated oval-shaped fluid density structure. There is free fluid in the pelvis. Pelvic inflammatory disease with tubo-ovarian abscess Pelvic inflammatory disease (PID) represents a common and potentially life-threatening disease among women of childbearing age, mostly occurring in their 2nd to 3rd decade (peak incidence: 20–24 years). This condition typically results from ascending infection of the female genital tract and is typically caused by Neisseria gonorrhoeae or Chlamydia trachomatis, although 40% of cases are associated with polymicrobial agents. PID usually begins with a cervicitis that subsequently extends to the endometrium and fallopian tubes; the infection may spread via tubal spillage to the peritoneum, leading to a local peritonitis. Tubo-ovarian abscess is the result of postinflammatory fusion of an infected fallopian tube and ovary (tubo-ovarian complex). Clinical diagnosis is often inaccurate, as patients may experience multiple nonspecific symptoms, including abdominal and pelvic pain, high fever, nausea, vomiting, vaginal discharge, uterine bleeding, dysuria, dyspareunia, and adnexal or cervical tenderness. Conversely, ˜35% of patients with PID have no noticeable symptoms. Laboratory findings are suggestive of infection such as leukocytosis, elevated erythrocyte sedimentation rate, and elevated C-reactive protein.
Clinical Presentation
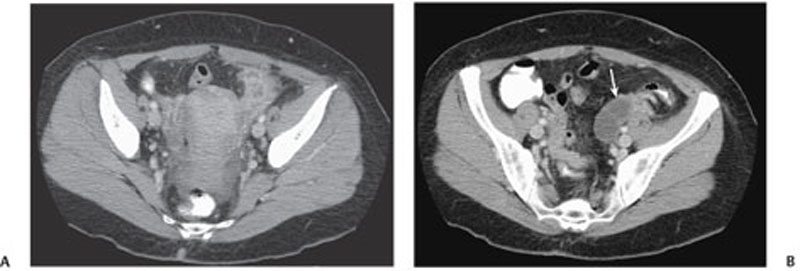
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Clinical Findings
Complications
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


