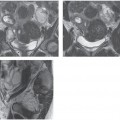
CASE 136 A 26-year-old woman presents with vaginal bleeding. She has a history of multiple miscarriages. Fig. 136.1 (A) Axial MR T2-weighted image demonstrates two uterine horns with a single cervix. Uterine zonal anatomy appears otherwise normal. A rounded T2 hyperintense focus is visualized within the cervix consistent with a nabothian cyst.(B) Axial MR T1-weighted fat-suppressed image obtained after the administration of intravenous gadolinium shows normal enhancement of the uterus. An axial magnetic resonance (MR) T2-weighted image (Fig. 136.1) demonstrates two uterine horns with a single cervix. The uterine zonal anatomy appears otherwise normal. A rounded T2 hyperintense focus is visualized within the cervix consistent with a nabothian cyst. An axial MR T1-weighted fat-suppressed image obtained after the administration of intravenous gadolinium shows normal enhancement of the uterus. Bicornuate uterus Uterovaginal (müllerian) anomalies result from alterations in the development or fusion of müllerian ducts and are associated with a high incidence of infertility, spontaneous abortion, fetal intrauterine growth retardation, preterm labor, and retained placenta; for this reason, most of these abnormalities are discovered in young adulthood or during pregnancy. The incidence is roughly estimated to range between 0.1 and 0.5% in the female population. Müllerian duct anomalies are commonly categorized into four classes according to embryology: Prompt identification of these anomalies is mandatory for the appropriate treatment of infertility and related symptoms.
Clinical Presentation
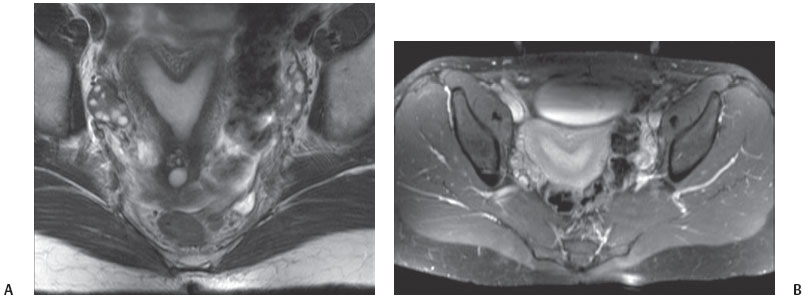
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Clinical Findings
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


