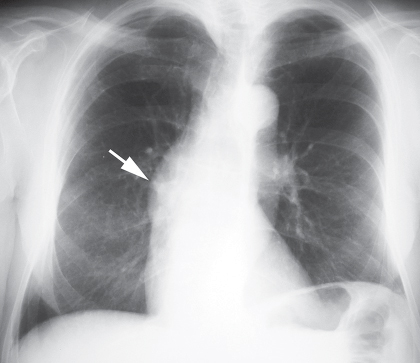
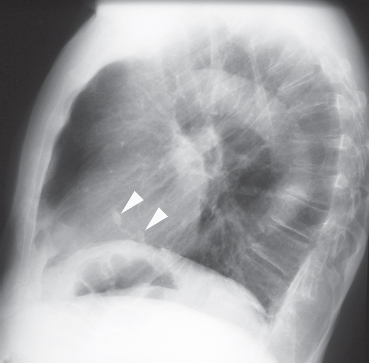
CASE 139 Asymptomatic 55-year-old man PA (Fig. 139.1) and lateral (Fig. 139.2) chest radiographs demonstrate dilatation of the ascending aorta (arrow) (Fig. 139.1) and dense calcification of the aortic valve (arrowheads) (Fig. 139.2). The heart size and pulmonary vascularity are normal. Aortic Stenosis; Bicuspid Aortic Valve • Hypertension The aortic valve has a tricuspid morphology with right, left, and posterior leaflets. In normal hemodynamics, systolic elevation of left ventricular pressure forces the valve open, and diastolic elevation of systemic pressure (relative to left ventricular pressure) forces it closed. Aortic stenosis refers to obstruction of antegrade blood flow between the left ventricle and the systemic circulation and may be valvular, supravalvular, or subvalvular (asymmetric septal hypertrophy). Aortic stenosis is a lesion of pressure overload, but almost always exhibits a component of secondary aortic insufficiency as calcium deposits on the stenotic valve often interfere with normal closure. Fig. 139.1 Fig. 139.2 (Images courtesy of Diane C. Strollo, MD, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania.) Congenital aortic stenosis may manifest with a unicuspid (patients under 15 years), bicuspid (patients 15–65 years), or tricuspid (patients over 65 years) aortic valve. However, over 95% of patients with congenital aortic stenosis have unicuspid or bicuspid aortic valves. The latter occur in 1.5% of live births, and aortic stenosis is the most common complication. Acquired aortic stenosis may occur as a sequela of rheumatic heart disease or as a degenerative condition in patients over 65 years of age.
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


