14 Imaging of Liver Tumors
Christopher P. Coppa
14.1 Introduction
This review will discuss the imaging features of commonly encountered malignant hepatic neoplasms. The computed tomography (CT) and magnetic resonance (MR) imaging appearances of hepatic metastases and primary hepatic neoplasms, including hepatocellular carcinoma (HCC) and cholangiocarcinoma (CCA), are summarized, with a focus on techniques for detection and patterns of enhancement using dynamic contrast-enhanced imaging. Further, CT and MR findings after locoregional therapy are reviewed, as is the application of these findings to different anatomic and functional-based treatment response models.
14.2 Technical Considerations
Multiphase dynamic contrast-enhanced imaging is the primary method used to characterize liver lesions on CT, and this technique also plays an important but not exclusive role in characterizing hepatic lesions on MR imaging. The patterns of enhancement observed in various hepatic lesions are the same on CT and MR imaging when extracellular contrast agents are administered. However, MR imaging can also use additional pulse sequences (e.g., T1-weighted, T2-weighted, and diffusion-weighted images) in conjunction with postcontrast images to better characterize lesions. As such, MR imaging is the imaging modality of choice for initial lesion characterization, whereas CT is generally reserved for patients who cannot undergo MR imaging. 1
Regardless of the modality used, dynamic contrast-enhanced liver imaging typically involves late arterial, portal venous, and delayed phases. While portal venous and delayed-phase images are typically acquired at fixed time points after the injection of contrast, the timing of the late arterial phase acquisition is usually tailored to the individual patient. Achieving satisfactory late arterial phase images requires optimization of the time delay between the administration of intravenous contrast material and the initiation of image acquisition. Fixed time-delay techniques are generally considered less reliable given variability in patient factors (such as cardiac output); therefore, bolus tracking or timing-bolus techniques are generally recommended. 2 , 3 , 4 High temporal resolution MR imaging performed with multiple arterial acquisitions may also be used to increase the likelihood of obtaining diagnostic arterial phase images. 5
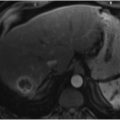
Meticulous timing of the arterial phase acquisition is crucial, as hypervascular tumors, including HCC and hypervascular metastases, demonstrate maximum enhancement during the late arterial phase. Radiographically, this phase is achieved when there is uniform contrast opacification of arteries and some early portal venous filling but an absence of hepatic vein opacification. Improper timing of the arterial phase may reduce the conspicuity of HCC and hypervascular metastases. Improper timing may involve imaging too early (i.e., the early arterial or angiographic phase, during which there is opacification of arteries but no portal or hepatic venous filling; ▶ Fig. 14.1) or imaging too late (i.e., when there is portal and hepatic venous opacification; ▶ Fig. 14.2). 6


The importance of well-timed dynamic contrast-enhanced imaging cannot be overstated. The Organ Procurement and Transplantation Network (OPTN) developed a policy in 2011 recommending that transplantation centers across the United States adopt certain technical specifications for dynamic contrast-enhanced imaging to optimize the diagnosis of HCC. 6 This stems from the fact that patients diagnosed with HCC are eligible for Model for End-Stage Liver Disease (MELD) exception points and may therefore gain higher priority on the liver transplant waiting list. 7 If the radiologic criteria for diagnosing HCC cannot be applied because of a technically insufficient study, the results of the study cannot be used to assign automatic exception points for transplant. 6 These OPTN technical specifications set minimum levels of functionality for CT and MR scanners and emphasize the importance of correct timing of image acquisition, especially for the late arterial phase.
14.3 Metastases
Metastases are the most common hepatic malignancies, occurring significantly more frequently than primary liver tumors. As such, most liver imaging is performed to evaluate metastases. 8
14.3.1 Enhancement Patterns
Liver metastases have different appearances depending on the histology of the primary tumor and can be broadly classified as hypovascular and hypervascular based on their enhancement patterns. 8 Contrast-enhanced CT and MR examinations can be tailored to assess these differences in enhancement. Although multiphasic contrast-enhanced imaging is routinely performed during every MR scan of the liver, multiphasic contrast-enhanced CT is not always performed because of the ionizing radiation associated with additional phases. Multiphasic CT imaging is indicated for the initial evaluation of an unknown liver mass (in a patient not eligible for MR imaging) and potentially for the surveillance of hypervascular malignancies, but this technique is generally not warranted in cases of hypovascular metastases, which can usually be assessed with a single-phase (i.e., portal venous phase) approach. Ultimately, the use of multiphasic CT imaging depends on the clinical scenario, and protocols for use vary among institutions.
Most metastases are hypovascular and are best visualized during the portal venous phase of enhancement, when enhancement is less than that of the background liver. Colorectal, lung, and gastric cancers classically produce hypovascular liver metastases. 8 These lesions have a “target” appearance created by an early complete ring of peripheral enhancement and a hypoenhancing center (▶ Fig. 14.3), followed by incomplete central progression on the delayed phase. 9

On CT, hypovascular metastases usually have attenuation greater than that of cysts (> 20 Hounsfield units) but less than that of the surrounding liver (▶ Fig. 14.4). One caveat is that the center of necrotic or mucin-containing metastases can mimic cysts on both CT and MR imaging. The presence of irregular margins or peripheral enhancement helps discriminate such lesions from benign hepatic cysts, which have no associated enhancement. 10 , 11

Hypervascular metastases (i.e., metastases predominantly with arterial blood supply) show enhancement greater than that of the background liver during the arterial phase (▶ Fig. 14.5). Hypervascular metastases usually originate from primary tumors such as neuroendocrine tumor, renal cell carcinoma, and melanoma. Breast cancer metastases are usually hypovascular but are sometimes hypervascular. 9

Diffuse hypervascularity is often present in smaller lesions, whereas peripheral ring enhancement is more characteristic of larger lesions. Some hypervascular metastases, especially lesions of neuroendocrine origin, demonstrate peripheral hypoenhancement or washout compared to the enhancement of the center of the lesion on the delayed phase. This finding is insensitive but highly specific for metastases. When present, it is a feature that can be used to distinguish small hypervascular metastases from hepatic hemangiomas, which retain contrast material on the venous phase. 9 , 10
14.3.2 Hepatocyte-Specific Contrast Agents
Thus far, the discussion has applied to enhancement patterns seen after the intravenous administration of extracellular CT and MR contrast agents, which lack hepatocyte uptake. Another type of MR contrast agent, referred to as a hepatocyte-specific agent, has dual pharmacokinetic behavior. Shortly after contrast injection, this agent behaves similarly to extracellular agents, diffusing from the vascular space into the interstitial space. However, unlike extracellular agents, it subsequently accumulates in hepatocytes and is partially excreted by the biliary system. The hepatobiliary phase succeeds the dynamic phase, and the timing of acquisition depends on the agent administered: 20 minutes for gadoxate disodium (gadolinium ethoxybenzyl diethylenetriamine pentaacetic acid [Gd-EOB-DTPA]) and 45 to 120 minutes for gadobenate dimeglumine (Gd-BOPTA). 1
Images generated during the hepatobiliary phase can be used to discriminate between normal liver (and lesions with functioning hepatocytes) and lesions lacking hepatocytes, thereby providing excellent lesion detection and liver-to-tumor contrast. Lesions with hepatocytes (such as focal nodular hyperplasia) have some degree of contrast accumulation on the hepatobiliary phase, and lesions without hepatocytes (such as metastases, cysts, and hemangiomas) lack uptake. Although the absence of contrast accumulation within a lesion on the hepatobiliary phase is a nonspecific finding in isolation, lesion characterization can be achieved when hepatobiliary phase findings are reviewed in conjunction with the other conventional MR sequences, including the dynamic contrast-enhanced portion of the study. 12
Gd-EOB-DTPA is particularly useful for detecting very small metastases (< 1 cm) and differentiating these lesions from focal nodular hyperplasia and hepatic cysts. Several studies have shown that MR imaging performed with hepatocyte-specific contrast depicts more liver metastases and improves lesion characterization when compared with CT. 13 For example, MR imaging with Gd-EOB-DTPA is superior to CT in detecting liver metastases from colorectal cancer; some consider this technique the preoperative imaging modality of choice in patients being considered for surgical treatment of such metastases. 14 Further, MR imaging with Gd-EOB-DTPA is more sensitive than positron emission tomography (PET)/CT for detecting liver metastases (▶ Fig. 14.6), especially lesions smaller than 1 cm. 15

14.3.3 Additional Magnetic Resonance Sequences
Although liver lesions can often be characterized as metastases based on CT or MR enhancement patterns alone, absolute characterization and quantification of metastases is most commonly performed with MR imaging because of the higher specificity gained by adding complementary pulse sequences, including T2-, T1-, and diffusion-weighted sequences. 1 This is especially important in the evaluation of small lesions that are often indeterminate on CT.
T2-Weighted Imaging
Most liver metastases have increased signal on T2-weighted images, with intensity similar to that of the normal splenic parenchyma (▶ Fig. 14.7) but less than the marked signal hyperintensity generated by hepatic cysts and hemangiomas. This degree of signal intensity is often observed in solid lesions and is not entirely specific for metastases but often indicates malignancy. One exception is mucinous metastases, which may have T2 signal intensity similar to that of a hemangioma because of their high water content. 16 Further, some less common metastases (e.g., lesions containing blood products, smooth muscle, calcification, or fibrotic components) may demonstrate low T2 signal. 17

T1-Weighted Imaging
Although most metastases are hypointense or isointense to the background liver on T1-weighted images, some metastases have T1 signal hyperintensity because of the presence of paramagnetic substances within the lesion. For example, some melanoma metastases have high T1 signal (▶ Fig. 14.8) because of the presence of melanin and extracellular methemoglobin. 8

Diffusion-Weighted Imaging
Diffusion-weighted imaging (DWI) is a functional MR technique that is useful for the identification and sometimes characterization of liver lesions based on lesion cellularity. Image contrast is dependent on differences in the mobility of water protons within various tissues, measured as the apparent diffusion coefficient (ADC). This technique is superior to T2-weighted sequences for the detection of liver metastases and is especially useful when gadolinium is contraindicated because of renal insufficiency or allergy. 18 , 19
Classically, highly cellular lesions (e.g., tumors) restrict the diffusion of water, which translates into high signal on high b-value DWI and low signal on the corresponding ADC map (▶ Fig. 14.9). In comparison, benign lesions typically permit greater diffusion of water molecules, resulting in decreased signal on high b-value images and high signal on the associated ADC map.

Applying these principles, DWI has a role in characterizing liver lesions as benign or malignant. However, it is important to remember that cystic, mucinous, and necrotic metastases may demonstrate high ADC values because of a lack of cellularity (less restriction of water), and some benign lesions (e.g., abscesses and focal nodular hyperplasia) may have low ADC values. As such, there is an overlap in the appearance (and corresponding ADC values) of benign and malignant lesions on DWI, and ultimate characterization often relies on findings from conventional MR sequences. 18 , 19
Related posts:
 9 Interventional Management of Benign Refractory Ascites
9 Interventional Management of Benign Refractory Ascites
 13 Acute Cholecystitis, Cholelithiasis, and Choledocholithiasis
13 Acute Cholecystitis, Cholelithiasis, and Choledocholithiasis
 15 Hepatocellular Carcinoma: Staging and Clinical Management
15 Hepatocellular Carcinoma: Staging and Clinical Management
 23 Yttrium-90 Radioembolization of Malignant Liver Tumors
23 Yttrium-90 Radioembolization of Malignant Liver Tumors
 27 Image-Guided Colorectal Obstruction Management
27 Image-Guided Colorectal Obstruction Management
 28 Obesity and Bariatric Embolization
28 Obesity and Bariatric Embolization
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


