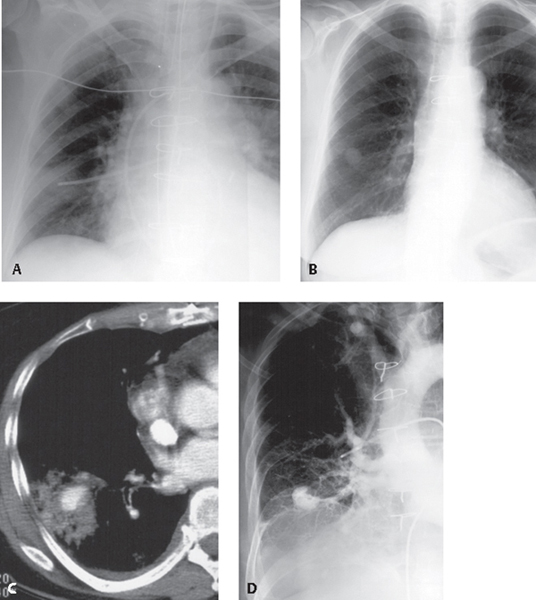
CASE 149 66-year-old man who had undergone a remote coronary artery bypass was readmitted with chest pain and had a new pulmonary artery catheter placed Coned-down AP chest radiograph (Fig. 149.1A) demonstrates a pulmonary artery (Swan-Ganz) catheter extending into the right lower lobe pulmonary artery; its tip projects beyond the right mid-clavicular line and is surrounded by focal indistinct ground glass opacity. Follow-up coned-down PA chest radiograph one week later (Fig. 149.1B) shows a new nodular opacity at the site of the previous catheter tip. Contrast-enhanced chest CT (Fig. 149.1C) reveals a focal collection of contrast enhancement (pseudoaneurysm) in the right lower lobe surrounded by parenchymal consolidation. Coned-down AP radiograph (Fig. 149.1D) obtained during pulmonary angiography illustrates a pseudoaneurysm in a right lower lobe pulmonary artery conforming to the previously demonstrated abnormality on chest radiography and chest CT. Fig. 149.1 Pulmonary Artery Catheter-Related Vascular Pseudoaneurysm; Right Lower Lobe Pulmonary Artery • Acute Invasive Aspergillosis (nodule with halo sign) Pulmonary artery aneurysms and pseudoaneurysms are uncommon and may be related to previous trauma, including iatrogenic events from improper placement of Swan-Ganz catheters. Other causes include blunt trauma, Behçet disease, infection (mycotic pseudoaneurysm), and Hughes-Stovin syndrome (recurrent thrombophlebitis, pulmonary artery formation and rupture).
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


