15 Normal Variants of the Skeleton and the Soft Tissues of the Hand
Nonpathologic variants of the skeleton of the hand include accessory sesamoid bones, coalescences and divisions of the carpal bones, and accessory bones. In contrast to malformations, these are not considered diseases and cause no functional disturbance. Diagnostically, these findings should always be differentiated from posttraumatic conditions. The most important variants of soft tissues of the hand are aberrant or accessory muscles. These are often asymptomatic and are discovered incidentally on MR images or during surgery.
Normal Variants of the Skeleton of the Hand
Sesamoid Bones
Sesamoids are located on the palmar side of the metacarpophalangeal and the distal interphalangeal joints. Their prevalence depends on their location, as listed in Table 15.1 .
Coalescence of the Carpals
Coalescence here refers to fusion of two carpal bones. Idiopathic coalescences, in which mostly two bones in the same carpal row are congenitally fused, are differentiated from postinflammatory or posttraumatic forms, which bridge the two carpal rows. Females and African Americans are more often affected by idiopathic coalescences.
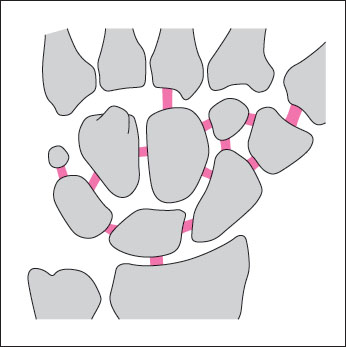
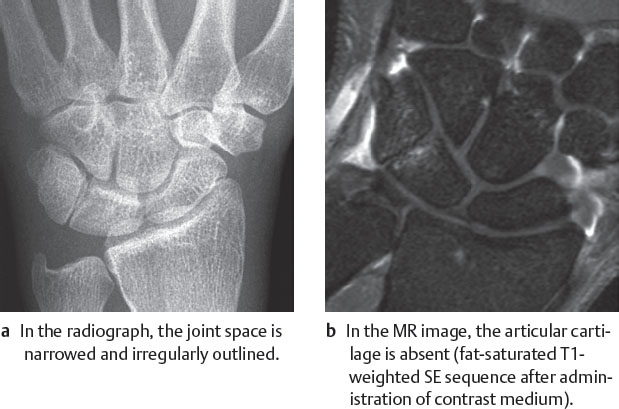
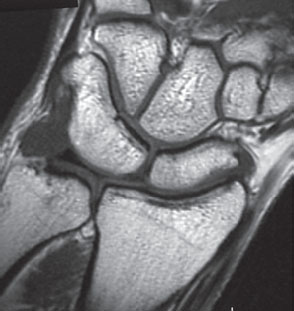
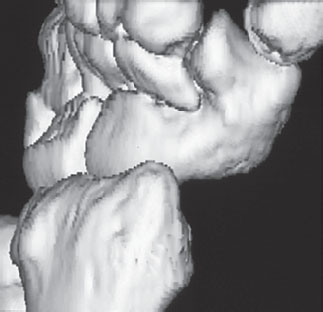
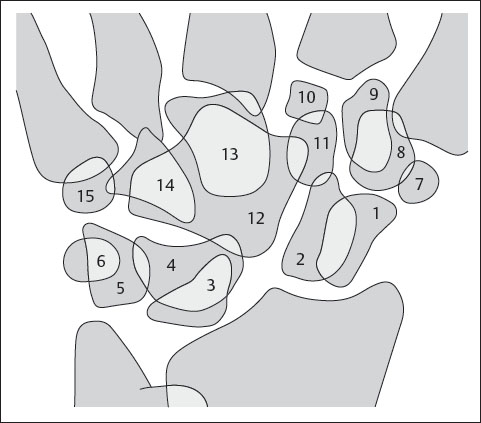
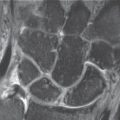
The different possible forms of carpal fusion are listed in Fig. 15.1 . The most common are fusions of the lunate and triquetrum ( Figs. 15.2–15.4 ), followed by fusions of the capitate and hamate ( Fig. 15.5 ). There are four different variations of lunotriquetral coalescence, which depend of the degree of the connecting synostosis or synchondrosis ( Table 15.2 ).
The remaining coalescences are very rare ( Fig. 15.6 ). When accessory elements fuse with adjacent carpals, they form defined exostoses.
Localization | Frequency(%) |
Sesamoid radial I | 95 |
Sesamoid ulnar I | 100 |
Sesamoid radial II | 50 |
Sesamoid radial III | 2 |
Sesamoid radial IV | 2 |
Sesamoid radial IV | <2 |
Sesamoid radial V | 3 |
Sesamoid radial V | 80 |
Sesamoid distal interphalangeal I | 70 |
Sesamoid distal interphalangeal II | <1 |
Sesamoid distal interphalangeal V | <1 |
Type | Description of Coalescence | Peculiarity |
I | Fibrous/fibrocartilaginous | |
II | Osseous incomplete | Distal notch |
III | Osseous complete | |
IV | Osseous complete | Further carpal anomalies |



|
Divided Carpals
Twofold or manifold divided carpal bones are very rare. In descending prevalence these involve the scaphoid, triquetrum, pisiform, trapezium, trapezoid, and capitate. Figure 15.7 lists possible divisions of the carpal bones. A typical bipartite scaphoid is shown in Fig. 15.8 .
When a divided carpal bone is discovered, a posttraumatic condition must be considered. This is especially true for the scaphoid, where fractures are often overlooked. Criteria for a truly bipartite scaphoid are summarized in Table 15.3.
A bipartite scaphoid supports the assumption that the division is congenital, but it does not constitute proof because bilateral scaphoid fractures or nonunions are also possible.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


