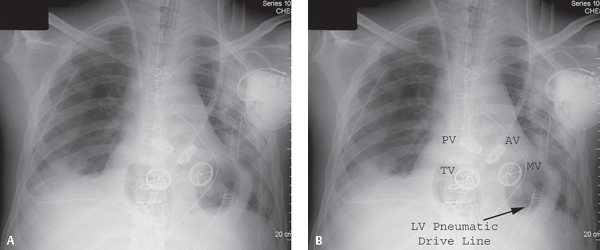
CASE 152 23-year-old man with non-ischemic cardiomyopathy and end-stage biventricular heart failure who has just undergone a sternal splitting thoracotomy and cardiac surgery as a bridge to orthotopic heart transplant AP chest radiographs without (Fig. 152.1A) and with accompanying annotations (Fig. 152.1B) demonstrate the normal postoperative appearance of a total artificial heart (TAH) implantation. Both native ventricles have been removed, as have all four native cardiac valves. The mechanical cardiac valves of the TAH are delineated (Fig. 152.1B). The air-containing diaphragms related to the artificial right and left ventricles of this pneumatic pulsatile device should not be confused with myocardial chamber air, pneumopericardium, or pneumomediastinum, and are an expected postoperative finding. The left ventricle pneumatic drive line is seen exiting through a port in the left upper quadrant and connects to a bedside console. Two mediastinal and bilateral pleural drains are present. Note the pre-existing ICD leads have been amputated. AV, mechanical aortic valve; MV, mechanical mitral valve; PV, mechanical pulmonic valve; TV, mechanical tricuspid valve. Total Artificial Heart (TAH) Implantation None Fig. 152.1 The total artificial heart (TAH) is presently used in the United States as a bridge for patients with end-stage biventricular heart failure awaiting heart transplantation. This mechanical device is a biventricular orthotopic pneumatic pulsatile pump with two separate artificial ventricles that replace the patient’s native ventricles. Each artificial semi-rigid polyurethane ventricle contains a seamless blood-contacting diaphragm, two intermediate diaphragms, an air diaphragm, and inflow and outflow mechanical valves. A flexible polyurethane-lined inflow connector is sewn to each atrial cuff of the recipient heart. Dacron graft outflow conduits are sewn to the patient’s native aorta and pulmonary artery, respectively. Wire-reinforced conduits covered with Dacron in the transabdominal wall pathways connect to longer drive lines and to an external console that controls the mechanical heart. The external console consists of two pneumatic drivers, one primary and one backup; transport batteries; air tanks; and an alarm and computer monitoring system. Heart rate, percentage of the cardiac cycle occupied by systole, and left and right driving pressures are manually controlled. The TAH is capable of pumping up to 9.5 L of blood per minute. A neopericardium created by Gore-Tex (W. L. Gore & Associates, Flagstaff, AZ) is placed about the TAH to diminish the formation of adhesions between the device and native pericardium and to expedite explantation when an orthotopic human heart becomes available.
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


