Conventional radiographs are the imaging modality of choice for the initial assessment of diseases of the lung or chest. Unfortunately, projection effects and a limited density resolution often restrict their informational value. Computed tomography (CT), particularly high-resolution CT, due to its high-contrast resolution and ability to depict even anatomical structures of submillimeter thickness, is regarded as a highly valuable complementary imaging method in the workup of pathologic processes of the thorax.
With the introduction of multislice CT and an isotropic voxel size of up to 0.4 m3, the image quality of multiplanar reconstructions has finally equaled that of transverse scans; thus, multi-planar assessment has become a standard approach in CT chest imaging. However, most diagnoses can still be made on simple 5-mm transverse slices reconstructed at 5-mm increments and acquired during inspiratory breath hold. A high-resolution CT scan, if needed, typically is done in addition to the 5/5-mm spiral scan, usually as a 1-mm slice thickness/10-mm increment sequence. Though this approach still represents the gold standard, on multislice CT scanners allowing for detector collimations < 1 mm, high-resolution images may alternatively be reconstructed directly from the spiral scan. Thus, the patient is exposed to a lower radiation dose without the two additional scans. However, a second CT scan may still be useful to identify air trapping, for example (i.e., when an additional expira-tory scan is needed). In such circumstances, the additional scan may be acquired as a 1-mm slice thickness/10-mm increment sequence. High-resolution CT typically is required in the presence of diffuse lung disease to detect and quantify subtle parenchymal changes and for morphological characterization, respectively.
On CT scans, attenuation values of normal lung parenchyma range from −700 to −900 HU. In the dependent portions of the lung, attenuation values usually are lower (less negative) due to orthostatic effects (i.e., increased blood flow). Because the most dependent portion of the lung on transverse CT images is the dorsal aspect of the lower lobe, this region physiologically often shows an ill-defined, up to 4-cm-thick band of higher attenuation. Likewise, attenuation values decrease (become more negative) when the amount of intrapulmonary air increases. This is observed during labored inspiration but also in several diseases with air trapping (e.g., emphysema).
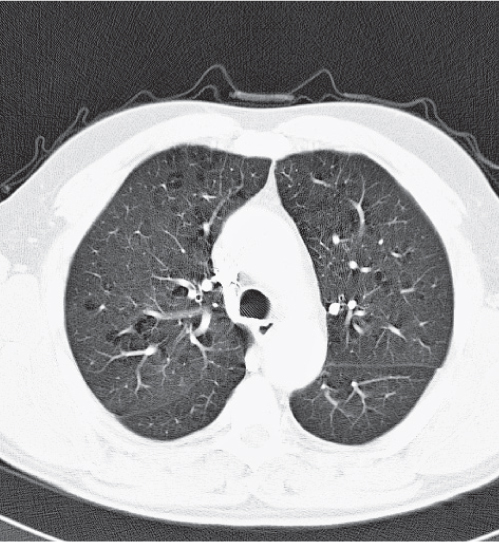
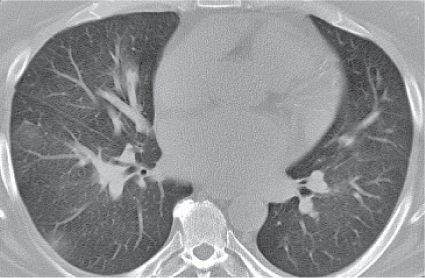
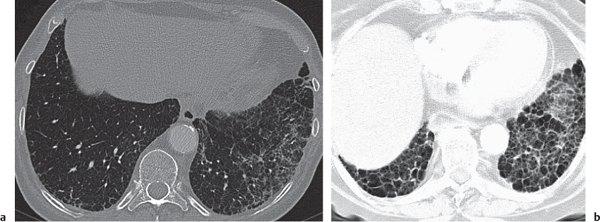
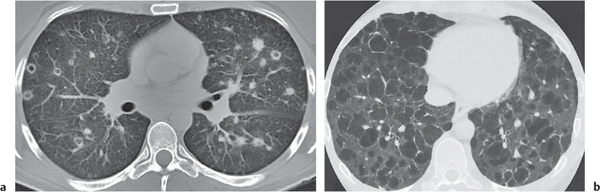
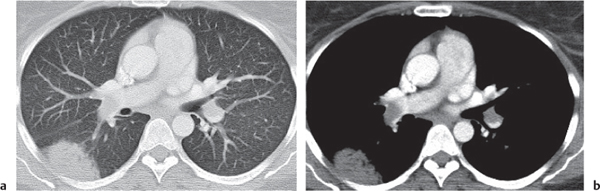
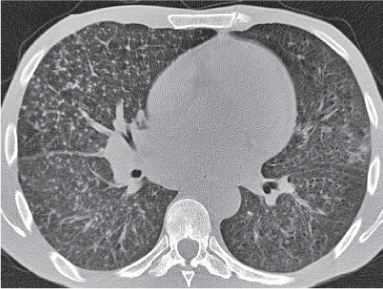
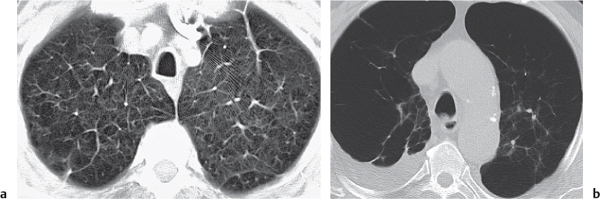
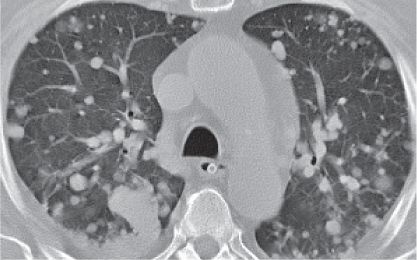
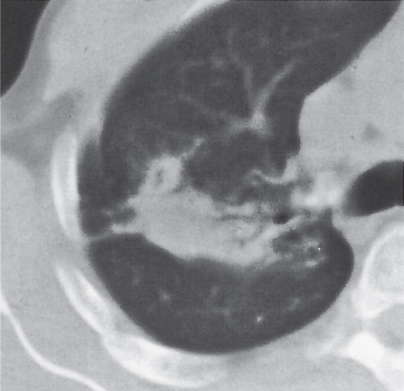
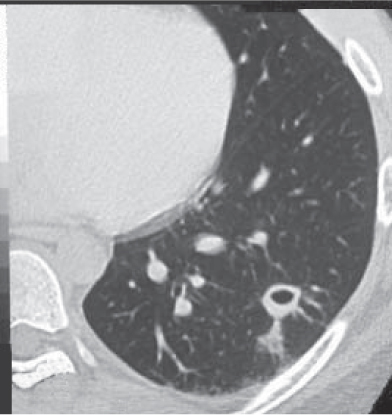
Bilateral hyperlucency is most often caused by chronic obstructive pulmonary disease (COPD) (Fig. 16.1). Other diseases typically associated with emphysema are alpha-1-antitrypsin deficiency, Marfan syndrome, Ehlers–Danlos syndrome, intravenous (IV) drug use, and human immunodeficiency virus (HIV) infection. Attenuation of emphysematous lung parenchyma amounts to values < − 950 HU. Primary bullous lung disease (vanishing lung) is an accelerated form of paraseptal emphysema found in young men who usually become symptomatic only if a spontaneous pneumothorax occurs. Pulmonary interstitial emphysema, a complication of enforced respiratory therapy, similarly presents with bilateral hyperlucent lungs, which is often associated with a pneumomediastinum. Reversible conditions of air trapping resulting in bilateral hyperlucency include asthmatic attacks and acute bronchiolitis, especially in children younger than 3 y. Other causes of a bilateral hyperlucent lung are decreased pulmonary blood flow due to thromboembolism (Westermark sign), pulmonary arterial hypertension, and a right-to-left shunt.
A unilateral or lobular hyperlucency is most often caused by air trapping due to extrinsic or intrinsic obstruction of a major bronchus. A unilateral hyperlucent lung with decreased lung volume despite air trapping, a small ipsilateral pulmonary hilus, and tubular or varicose bronchiectasis is diagnostic of the Swyer–James or Macleod syndrome. Compensatory emphysema is evident in the remaining lung after lobectomy or due to lobular atelectasis. Other causes of unilateral hyperlucency are one-sided emphysema/thromboembolic disease and rare congenital conditions, such as a hypogenetic lung, absent pulmonary artery (usually right), anomalous origin of the left pulmonary artery, and congenital lobular emphysema (usually upper or middle lobe), as well as scimitar syndrome. The latter is a combination of a hypoplastic hyperlucent right lung, small ipsilateral hilus, right shift of the heart and mediastinum, and a partial anomalous pulmonary venous return resembling a scimitar.
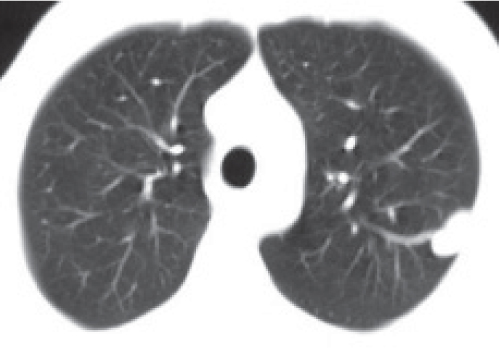
Normal major and minor fissures are usually not visible on CT scans, but their location can be assumed from a 2- to 3-cm-thick band of hyperlucent lung tissue, corresponding to relatively avascular parenchyma on each side of the fissure. Occasionally, a poorly defined ribbonlike zone of increased density is evident in the avascular area adjacent to the fissure, caused by volume averaging of the latter. In high-resolution CT, the fissures are usually visible as pencil-thin white lines.
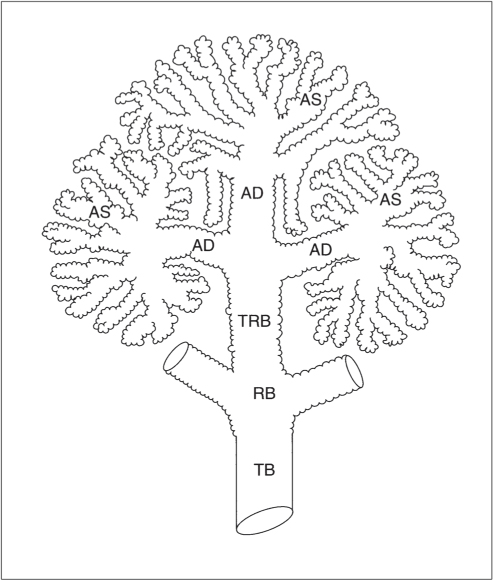
The pulmonary acinus (Fig. 16.2) is defined as the portion of lung distal to a terminal bronchiole and consists of respiratory bronchioles, alveolar ducts, alveolar sacs, and alveoli. The primary pulmonary lobule comprises all alveolar ducts, alveolar sacs, and alveoli together with their accompanying blood vessels, nerves, and connective tissues distal to the last respiratory bronchiole. The secondary pulmonary lobule is defined as the smallest discrete portion of lung that is surrounded by a connective tissue septum. It is composed of 3 to 5 terminal bronchioles or 30 to 50 primary lobules. It has an irregular polyhedral shape and ranges from 1 to 2.5 cm in diameter. On high-resolution CT scans, the secondary pulmonary lobule can be identified in both normal and pathologic states. It is surrounded by interlobular septa containing the peripheral tributaries of pulmonary veins and lymphatics. Because of the hydrostatic dilation of the intraseptal veins, the septa are most prominent in the dependent portions of the lung. Subtle changes of the secondary pulmonary lobule are first seen in the subpleural space of dependent lung portions.
Even on high-resolution CT scans terminal bronchioles and accompanying pulmonary arterioles are only rarely evident in healthy individuals. If visible, they appear as small dots or tiny branching structures in the centers of secondary lobules and are often referred to as centrilobular arteries and bronchioles.
Fig. 16.1 Panlobular emphysema. Bilateral hyperlucent lungs are evident with rarefaction of the peripheral pulmonary structures and relative prominence of central pulmonary vasculature.Fig. 16.2 Pulmonary acinus topography. The pulmonary acinus begins at the termination of the terminal bronchiole (TB) and measures ~8 mm at its widest diameter. Alveoli are tiny outpouchings found in the walls of an acinus.
AD
alveolar duct
AS
alveolar sac
RB
respiratory bronchiole
TRB
terminal respiratory bronchiole
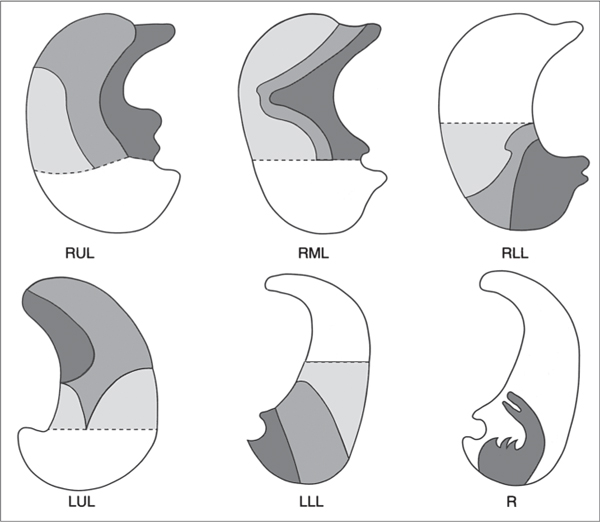
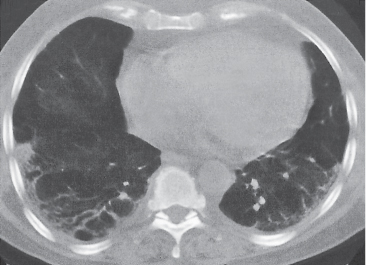
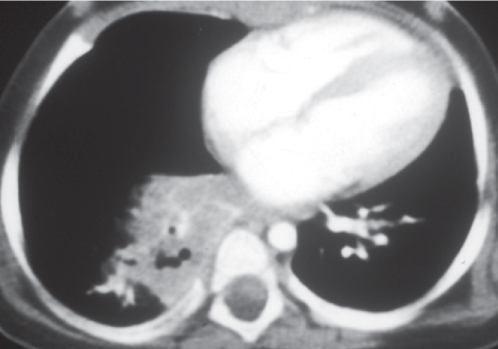
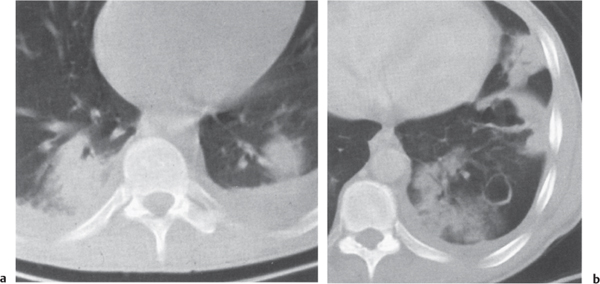
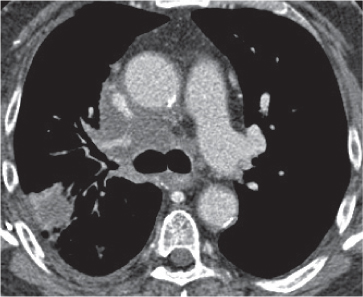
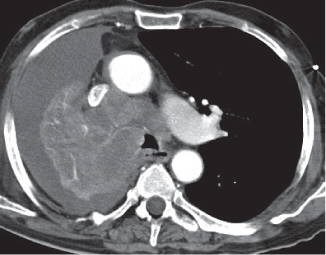
An increase in lung density occurs when air is replaced by liquid or solid material. A partially hyperdense lung lobule is found in early atelectasis and a completely collapsed lobule in atelectasis. The hallmarks of atelectasis are a loss in lung volume and a displacement of fissures (Fig. 16.3). The upper lobes collapse upward, medially, and anteriorly. A totally collapsed right upper lobe may eventually simulate an anterior paramediastinal mass. A right middle lobe collapse appears as a wedge-shaped density, with one side of the wedge abutting the mediastinum. The lower lobes collapse medially and inferiorly, maintaining contact with the posterior mediastinum.
Atelectasis may be divided into obstructive and nonobstructive forms. Obstructive (resorption) atelectasis occurs when the communication between the trachea and the lung periphery is obstructed by either an endobronchial lesion or extrinsic compression. The cause of obstruction is often identified on CT scans. The collapsed airless lung parenchyma distal to the obstruction is of soft tissue density, obliterating normal vascular structures. Bronchi are typically fluid-filled and thus air bronchograms are usually absent.
Nonobstructive atelectasis forms include relaxation, compression, round, adhesive, and cicatrization.
Relaxation (passive) atelectasis is observed in the presence of a pneumothorax or pleural effusion causing retraction of the lung from the chest wall toward the hilum. Compression atelectasis refers to the loss of lung volume adjacent to a large pulmonary or pleural space-occupying lesion.
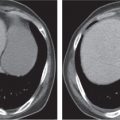
Round (helical) atelectasis (labeled R in Fig. 16.3) is caused by contracting pleural fibrosis, resulting in compression and often folding of contiguous lung parenchyma. It is associated primarily with asbestos-related pleural disease and is most commonly located in the posterior portion of a lower lobe. The characteristic CT appearance consists of a rounded subpleural opacity that is densest at its periphery. The bronchovascular bundle entering the lesion appears curvilinear (“comet tail” sign) and often contains an air bronchogram. Linear bands radiating from the mass into the lung parenchyma are also characteristic (“crow’s feet”).
In adhesive atelectasis, alveolar collapse occurs in the presence of patent airways and is likely caused by a lack of surfactant. It is found in respiratory distress syndrome of the newborn, acute radiation pneumonitis, and viral pneumonia.
Cicatrization (scar) atelectasis is associated with pulmonary fibrosis that may be localized or generalized. Localized disease is the sequela of chronic infection (e.g., tuberculosis) or inflammation (e.g., radiation). In these conditions, parenchymal fibrosis results not only in atelectasis, but also by traction on airway walls in bronchiectasis. The combination of severe loss of volume associated with extensive air bronchograms in normal or dilated bronchioles is characteristic.
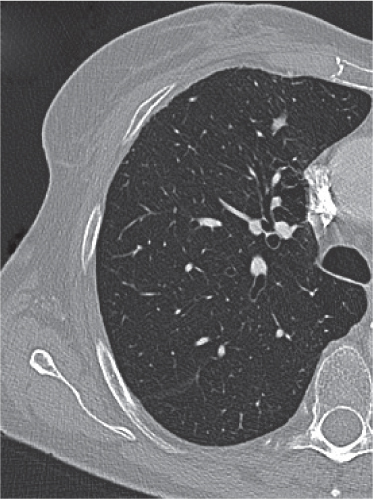
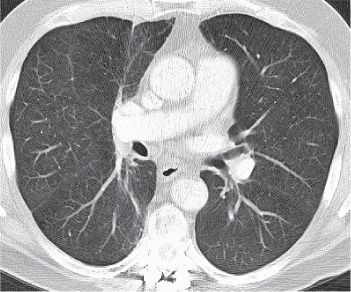
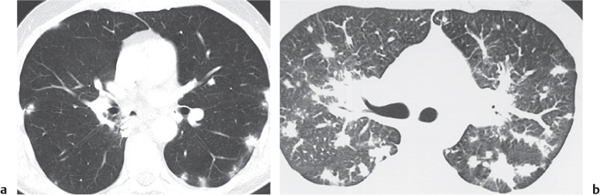
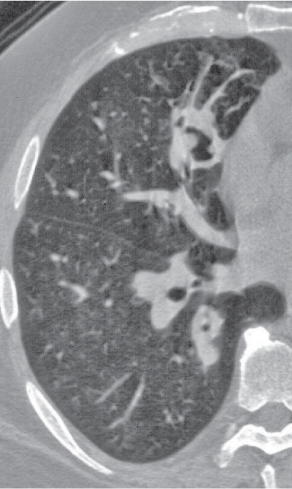
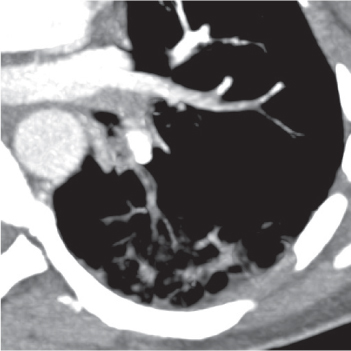
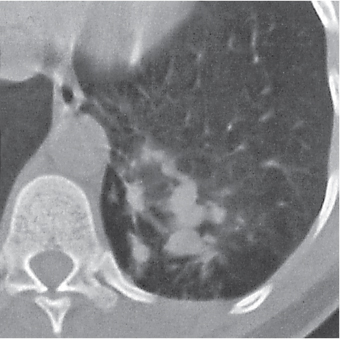
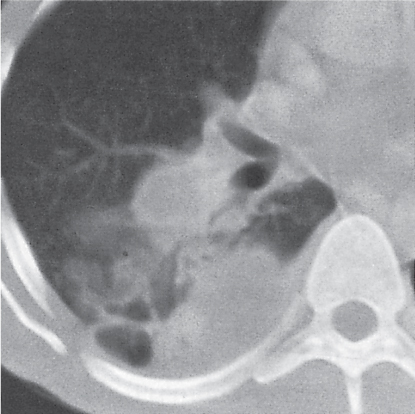
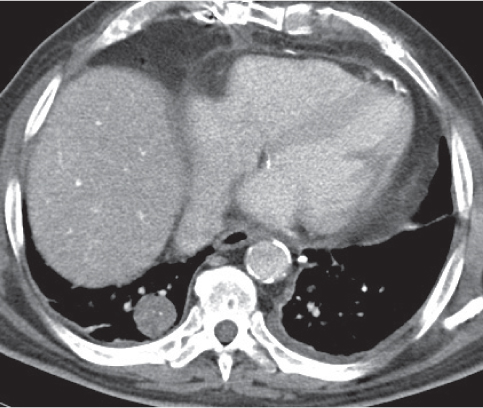
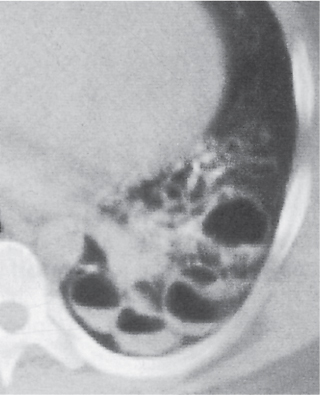
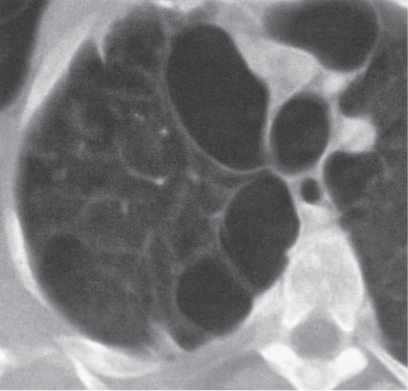
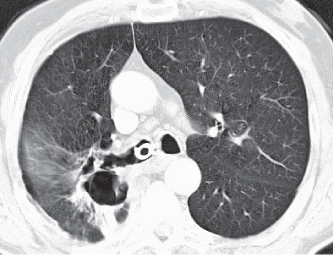
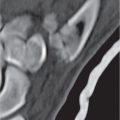
Bronchiectasis (Fig. 16.4) is an irreversible bronchial dilation and, depending on the severity of the disease, can be classified into cylindrical, varicose, and cystic forms. Cylindrical (tubular) bronchiectasis is characterized by uniform mild dilation of the bronchi; in varicose bronchiectasis, the bronchial dilation is further increased and alternates with areas of localized constriction; in cystic (saccular) bronchiectasis, the bronchial dilation increases progressively toward the periphery, resulting in cystic spaces measuring up to a few centimeters in diameter.
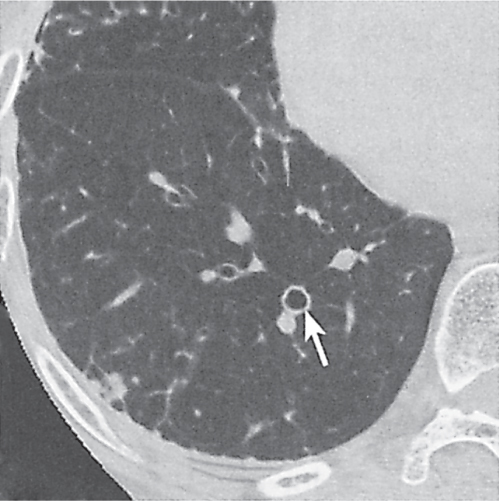
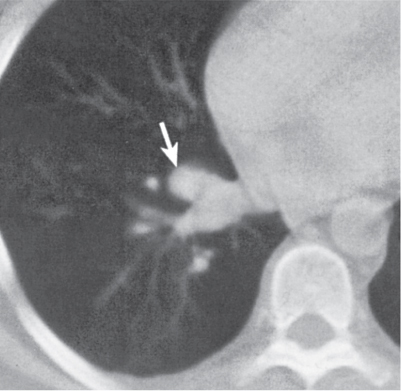
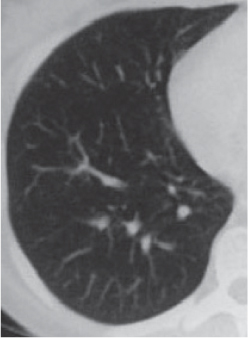
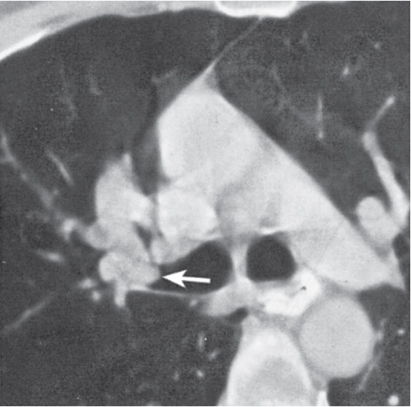
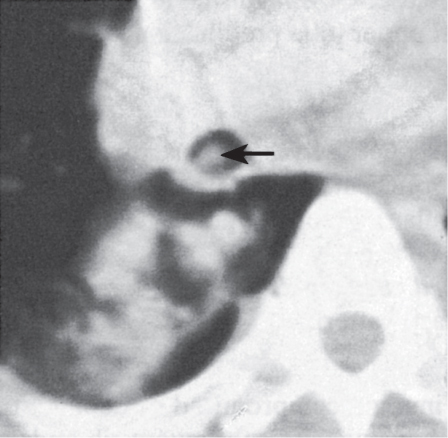
High-resolution CT is more accurate than CT in the diagnosis of bronchiectasis and has completely replaced bronchography. Cylindrical bronchiectases are recognized on CT as dilated thick-walled bronchi extending toward the lung periphery, whereas normal intraparenchymal bronchi are usually not visualized in the lung periphery. If cut perpendicular to their longitudinal axis, bronchi appear as ring-shaped bronchiectases accompanied by a much smaller pulmonary artery branch, producing a characteristic “signet ring” sign (Fig. 16.5). Bronchiectases may be filled completely with secretions or mucus, evident as large homogeneous tubular structures within the lung periphery. More advanced varicose bronchiectasis assumes a beaded configuration. Cystic bronchiectasis presents as thick-walled cystic spaces measuring up to 2 cm and often grouped together in a cluster. Fluid levels of varying sizes within these cysts are often evident and characteristic.
Fig. 16.3 Atelectasis. Patterns of progressive atelectasis pattern are shown for the right upper lobe (RUL), right middle lobe (RML), right lower lobe (RLL), left upper lobe (LUL), and left lower lobe (LLL). The dashed line presents the pertinent interlobular fissure in a normal position. Characteristic features of a round atelectasis (R) include a “comet tail” and “crow’s feet.”
Acquired bronchiectasis is the late sequela of bronchial wall damage. Diseases that predispose to bronchial wall infection and subsequent bronchiectasis formation include immunologic deficiency states such as agammaglobulinemia, chronic granulomatous disease, and allergic pulmonary aspergillosis.
In children, typical underlying diseases are measles, pertussis, and bronchiolitis obliterans, the latter often resulting in the Swyer–James syndrome. Bronchiectases are also a constant feature in cystic fibrosis and Kartagener syndrome (i.e., dyskinetic endobronchial cilia).
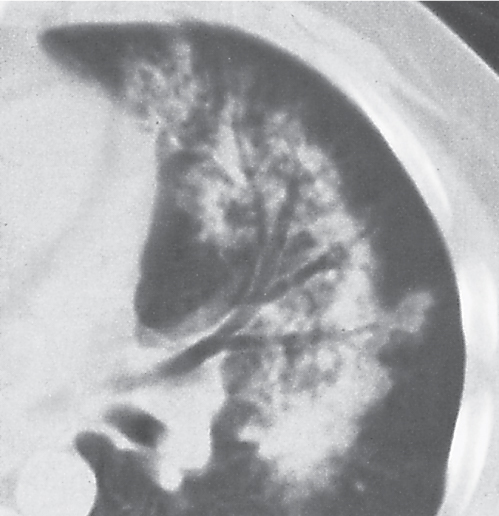
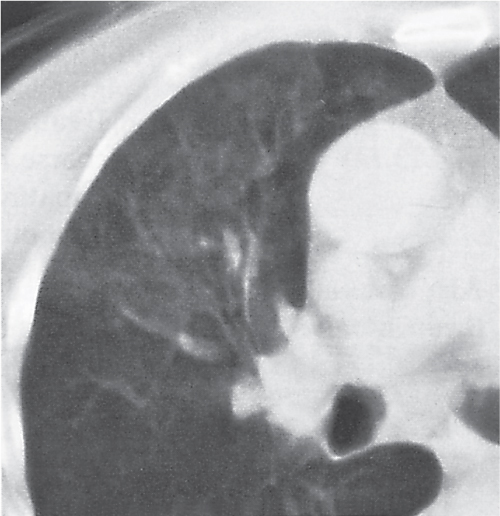
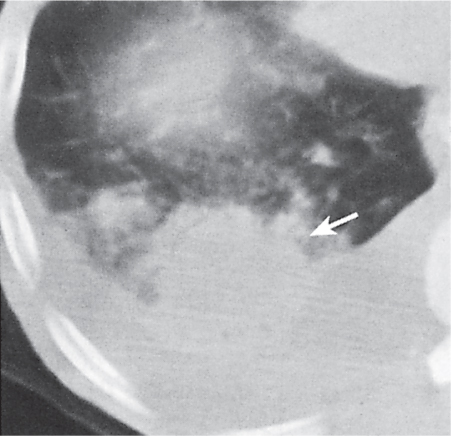
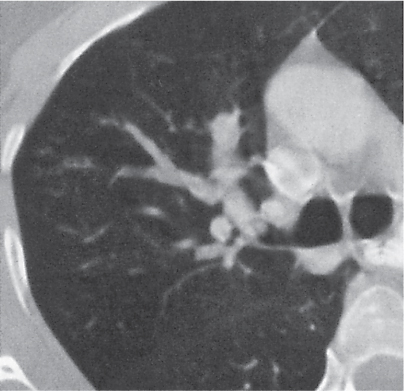
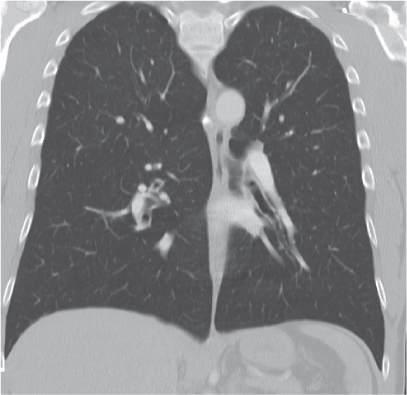
Fig. 16.4 Bronchiectasis. View of cylindriform bronchiectasis (parahilar) in the middle lobe of the right lung.Fig. 16.5 “Signet ring” sign. A cylindrical bronchiectasis viewed end on with the accompanying considerably smaller pulmonary artery branch produces the characteristic “signet ring” sign (arrow).
In adults, bronchiectases are typically associated with chronic aspiration, inhalation of toxic fumes, extrinsic and intrinsic bronchial obstruction (e.g., neoplasms or aspiration of foreign bodies), and emphysema.
Cicatricial (traction) bronchiectases develop as a result of retractile forces of the fibrotic lung on the bronchial wall and are observed in chronic tuberculosis, radiation pneumonitis, and some interstitial diseases such as sarcoidosis. Congenital abnormalities of the bronchial wall such as bronchomalacia are other, though rare, causes of traction bronchiectasis.
Chronic bronchitis is a clinical diagnosis based on excessive mucus production. On high-resolution CT, concentric bronchial wall thickening (“tram lines”) without bronchial dilation or the signet ring sign (as characteristic of bronchiectasis) is evident. These findings correspond to prominent lung markings or the “dirty chest” appearance of a lung seen on plain film radiography.
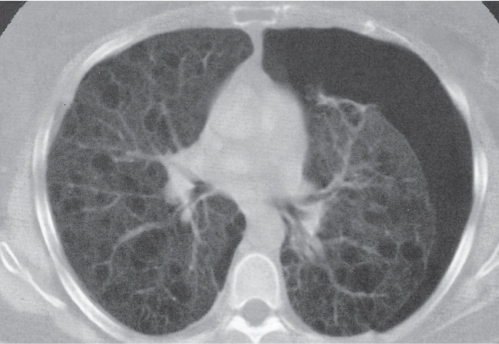
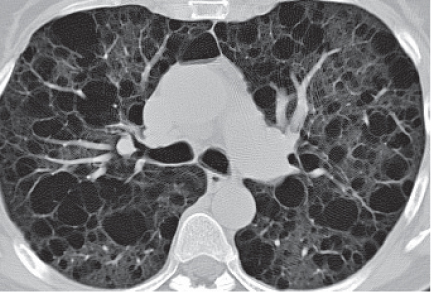
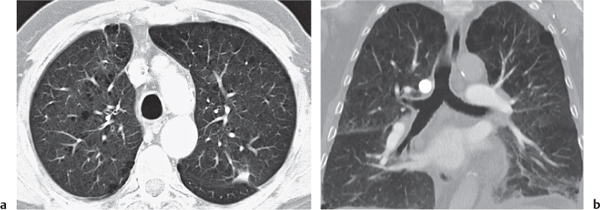
Emphysema (Fig. 16.6) is defined as an absolute permanent enlargement of any or all parts of the acinus associated with destruction of alveolar parenchyma but without fibrosis. It is a typical end-stage of COPD, a state of irreversibly obstructed airways without known mechanism, but it is also observed in patients with asthma, bronchiolitis, and alpha-1-antitrypsin deficiency. COPD has a male predominance (~10:1), and cigarette smoking is a major factor.
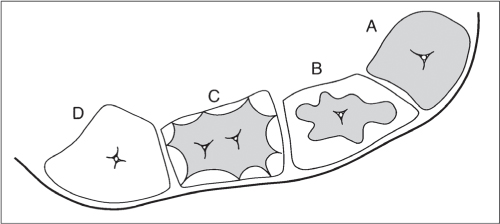
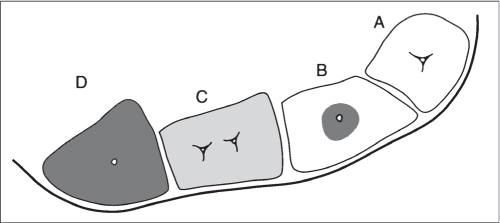
Four different types of emphysema are recognized: centrilobular, panlobular or panacinar, paraseptal, and irregular (Fig. 16.7).
In centrilobular emphysema, the respiratory bronchioles (the central or proximal portions of the acinus) are destroyed. It is observed primarily in the upper lung lobes and is commonly associated with smoking. CT findings range from scattered punctate dark holes via a moth-eaten pattern to larger areas of destroyed lung. Pulmonary vascular pruning and distortion are evident in more advanced stages.
In panlobular (panacinar) emphysema, the acinus and secondary lobules are uniformly destroyed, leading to a homogeneously distributed diminishment of the interstitium without zonal preference. On CT, widespread areas of low attenuation are characteristic. However, despite some differences in the distribution patterns, it is often impossible to differentiate a panlobular from an advanced centrilobular emphysema. In addition, differentiation between normal and diseased lung often is difficult. Panlobular emphysema is characteristic for alpha-1-antitrypsin deficiency, but it can also be found in smokers.
Paraseptal emphysema selectively involves the alveolar ducts and sacs in the periphery of the acinus or lobules. It is characteristically seen adjacent to the pleura and interlobular septa. It may represent an early form of bullous lung disease that may progress to bullous emphysema. Typical findings on CT scans are subpleural emphysematous spaces < 5 mm and larger subpleural bullae, both usually in the vicinity of the mediastinal pleura. Paraseptal emphysema is limited in extent and usually not associated with clinical disease, with the exception of a spontaneous pneumothorax.
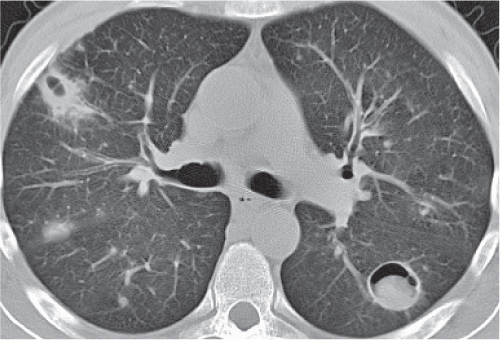
Fig. 16.6 Emphysema. Hyperlucent lungs with numerous black holes (small bullae). Also seen is a concomitant left pneumothorax.Fig. 16.7 Emphysema pattern. Schematic display of four secondary pulmonary lobules with barely visible centrilobular arteries and bronchioles. Normal secondary pulmonary lobule (A). Centrilobular emphysema (B). The respiratory bronchi (central or proximal portions of the acinus) are destroyed. Paraseptal emphysema; only alveolar ducts and sacs (peripheral portion of the acinus) are destroyed (C). Panlobular (panacinar) emphysema; note that the acinus and secondary lobule are destroyed in full (D).
Irregular (paracicatricial or scar) emphysema is always associated with localized (e.g., tuberculosis) or generalized pulmonary fibrosis (e.g., sarcoidosis and pneumoconiosis). Clinical abnormalities in this form of emphysema are mainly related to the underlying lung disease.
Bullae are frequently associated with emphysema but may also be found as a localized process in otherwise normal lungs (primary bullous disease). A bulla is defined as an air-filled thin-walled (“hairline”) intrapulmonary cavity > 1 cm in diameter.
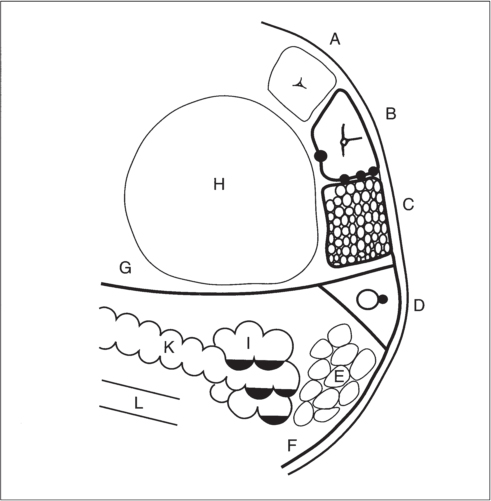
The pulmonary interstitium is the supporting structure of the lung and can be divided into two compartments: (1) the central or axial interstitial space, consisting of the connective tissue surrounding major airways and pulmonary vessels, and (2) the peripheral interstitial space, including the connective tissue of interlobular septa, as well as around the centrilobular arterioles and bronchioles. From an anatomical point of view, any distinction between the central and peripheral interstitium is arbitrary. However, in high-resolution CT, several interstitial diseases are first seen in the peripheral (subpleural) but not in the central interstitial spaces (Fig. 16.8).
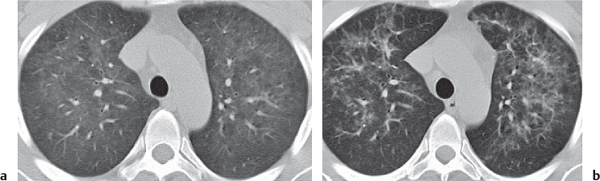
A key finding of interstitial lung disease is thickening of inter-lobular septa (reticular thickening), primarily visible in the peripheral (i.e., subpleural and basal) space. Normal interlobular septa are usually below the spatial resolution of high-resolution CT. Depending on the underlying disease, other typical findings include nodular and nonnodular thickening of interlobular septa, centrilobular nodules, and honeycombing.
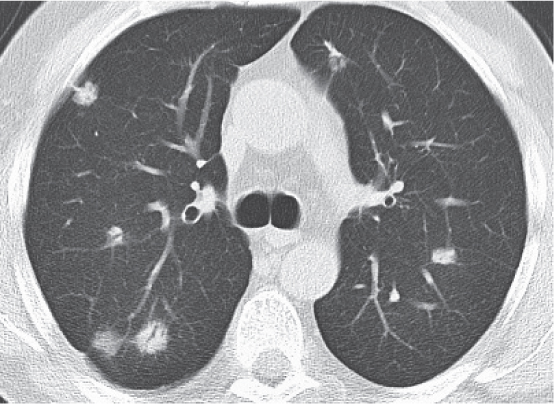
Nodular thickening of interlobular septa and peribronchial noduli are commonly associated with interstitial diseases affecting the lymphatics, such as metastatic spread (i.e., lymphangiosis carcinomatosa), sarcoidosis, and silicosis. Nonnodular thickening is more typical of infectious diseases or fibrosis.
Centrilobular noduli may show a bronchocentric or a lymphatic pattern.
A bronchocentric pattern affects the acinus, including all structures distal to the end-terminal bronchiole. It is initiated through inhalation of particles and subsequent mural infection/inflammation. High-resolution CT shows multiple < 5-mm nodules, often Y or V shaped (“tree-in-bud” sign). The peripheral subpleural space typically is spared (differential diagnosis to lymphatic pattern). Expiratory scans show mosaic perfusion (thickening of paper-thin bronchioles leading to regional air trapping). Differential diagnoses include respiratory bronchiolitis, viral bronchiolitis, hypersensitivity pneumonitis, coal workers’ pneumoconiosis, COPD, and centrilobular emphysema.
Fig. 16.8 Peripheral interstitial disease pattern. Normal secondary pulmonary lobule (A). Thickening of the interlobular septa, which may be nodular (B); note also the thickening of the centrilobular artery and bronchiole. Honeycombing (C). “Signet ring” sign (D). Also evident are tubular bronchiectasis and the adjacent pulmonary arterial branch cut perpendicular. Thin-walled cystic spaces (E), which may become confluent. Thickened subpleural line (F). Parenchymal bands or scars terminating in interlobular septa at the pleural surface (G). Bulla (H). Cystic bronchiectases (I), commonly with fluid levels. Varicose bronchiectasis (K). Tubular bronchiectasis (L).
The lymphatics form two pulmonary networks: a central network along arteries and airways down to the respiratory bronchioles and a peripheral network along pulmonary veins, interlobular septa, and pleura. In the lymphatic pattern, centrilobular nodules < 5 mm are found in a peribronchiolar, periseptal, and subpleural distribution. However, it may still be initiated through inhalation of particles; thus, differentiation between a bronchocentric and lymphatic pattern often is difficult. Involvement of the subpleural space is highly indicative of the latter. A lymphatic pattern is observed in diseases with a predominantly lymphatic spread, including sarcoidosis, lymphangiosis carcinomatosa, metastatic spread, pneumoconiosis, lymphocytic inter-stitial pneumonia (LIP), and cardiogenic pulmonary edema.
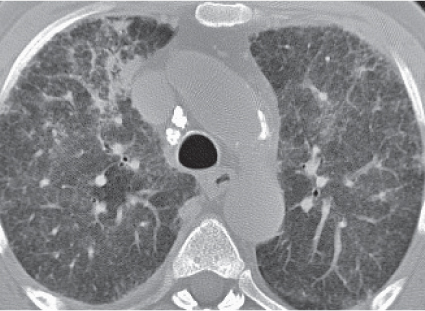
Honeycombing is an advanced stage of pulmonary interstitial fibrosis. Uniform cystic spaces ranging in diameter from 5 to 10 mm with thick walls are characteristic.
Honeycombing is caused by a limited number of diseases, including idiopathic pulmonary fibrosis, scleroderma, rheumatoid lung disease, eosinophilic granuloma, lymphangioleiomyomatosis, pneumoconiosis (e.g., silicosis, coal workers’ pneumoconiosis, and asbestosis), and sarcoidosis. It is particularly evident in both lower lobes except for eosinophilic granuloma, sarcoidosis, and silicosis, which show upper zone predominance of honeycombing. In idiopathic pulmonary fibrosis and scleroderma, the lung volume is characteristically decreased, whereas in pneumoconiosis and sarcoidosis, it is increased. This is due to a coexistence of pulmonary fibrosis and obstructive airway disease with cystic spaces varying from 1 to 10 cm in diameter.
Extensive fibrosis results in architectural distortion. Occasionally, traction bronchiectasis and conglomerate masses (progressive massive fibrosis [PMF]) preferentially located in the upper lobes may occur, especially in pneumoconiosis and sarcoidosis.
Typically observed in patients with asbestosis, but also those with pulmonary fibrosis and lymphangitic carcinomatosis, are thin subpleural lines, 2 to 10 cm long, paralleling the chest wall (curvilinear subpleural lines), as well as nontapering bands of fibrous tissue radiating from the lung periphery.
Central peribronchial interstitial edema, infiltrates, and fibrosis manifest on CT as apparent bronchial wall thickening. Irregular and serrated thickening of bronchi and vessels suggests fibrosis, whereas a smooth thickening of these structures favors edema and infiltrates. Besides these edematous and infectious processes, central interstitial thickening is associated with lymphangitic carcinomatosis, lymphoma, and sarcoidosis.
In air-space (alveolar) disease, the air in peripheral airways is replaced by fluid, cells, or solid substances, resulting in an increased regional lung density.
The following conditions may be underlying causes: (1) low osmotic blood pressure (e.g., hypoproteinemia), (2) high capillary blood pressure (e.g., congestive heart failure), (3) defective alveolocapillary barrier (e.g., shock, lung contusion, and inhalation of noxious gases), (4) aspiration, (5) secretion of abnormal substances (e.g., cystic fibrosis), (6) deposition of abnormal substances (e.g., alveolar proteinosis), (7) invasion of cells (e.g., infectious and inflammatory conditions), and (8) intra-alveolar cell growth (e.g., neoplasm).
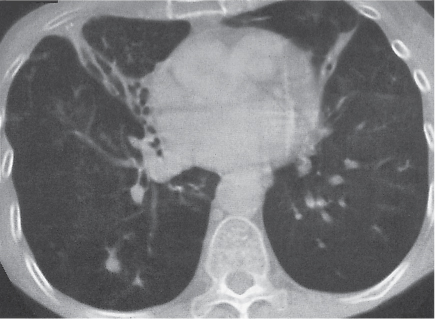
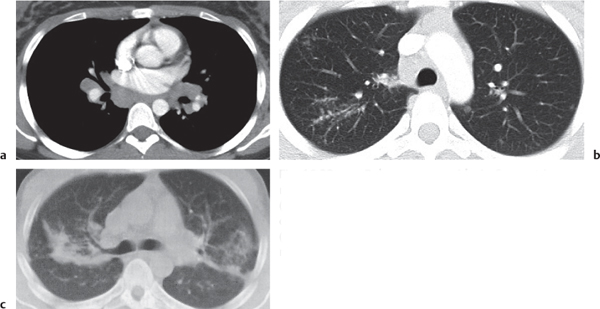
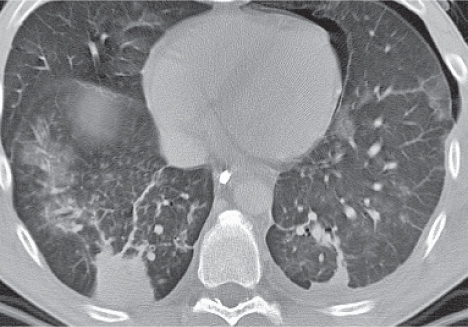
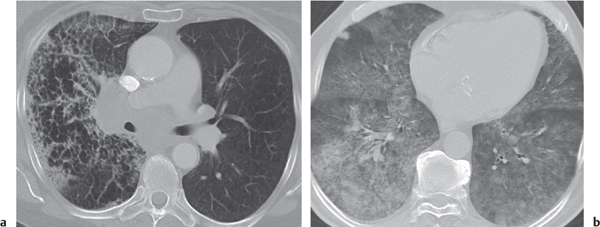
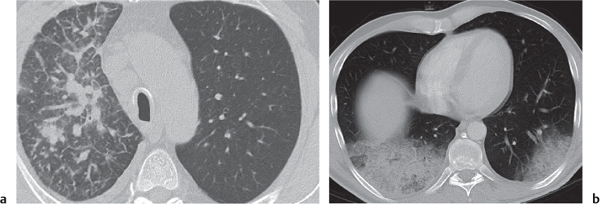
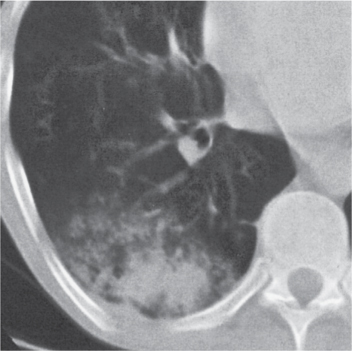
As indicated above, air-space disease (Fig. 16.9) presents in its early stages as poorly defined bronchocentric nodularities, measuring about 0.5 to 1 cm in diameter. With progression of the disease, these nodules coalesce and form larger areas of consolidation, obscuring pulmonary vessels and causing characteristic air bronchograms (Fig. 16.10). However, air bronchograms are also encountered in atelectasis and, rarely, in extensive interstitial disease, such as sarcoidosis.
Diffuse air-space disease tends to involve central portions of the lungs, whereas diffuse interstitial processes are predominantly observed in the lung periphery. CT attenuation values do not permit differentiation between different air-space consolidations. Relatively high attenuation values are found in acute pulmonary hemorrhage and chronic renal failure, possibly due to dystrophic microcalcifications.
Diffuse interstitial and/or micronodular densities with increased attenuation are associated with mitral stenosis or other conditions with chronically elevated left atrial pressure, as well as with healed disseminated infections, such as tuberculosis, histoplasmosis and varicella pneumonitis, silicosis, radiopaque dust inhalation, amyloidosis, and alveolar microlithiasis. Occasionally, they are also found in pulmonary fibrosis (idiopathic or long-term busulfan therapy), deposition of iodine-containing drugs (e.g., amiodarone therapy or postlymphography), idiopathic pulmonary hemosiderosis, and Goodpasture syndrome.
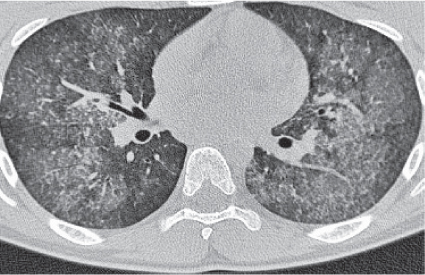
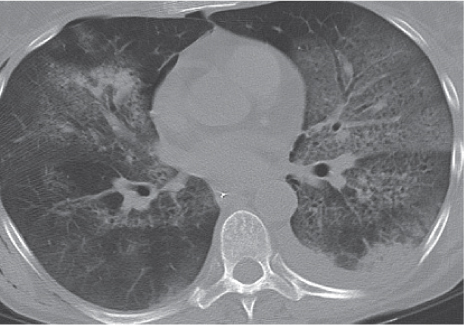
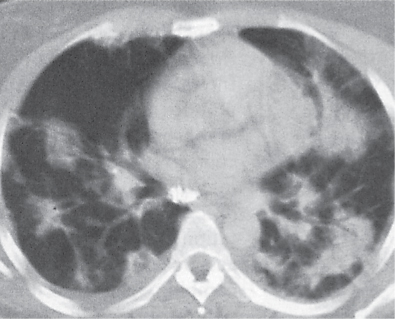
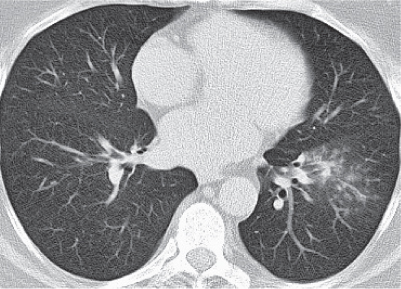
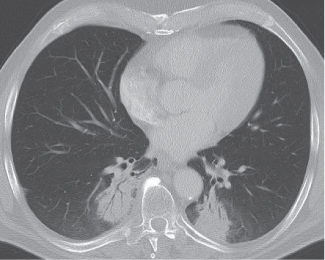
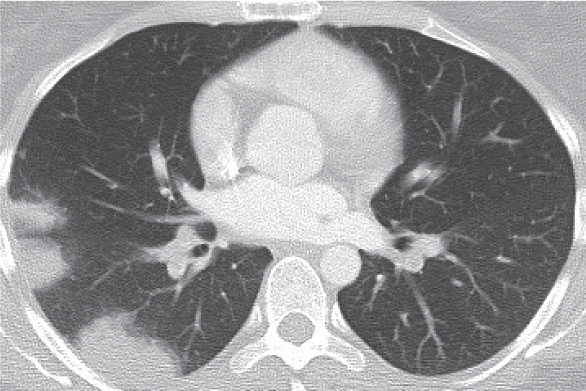
Fig. 16.9 Air-space disease pattern. Normal secondary pulmonary lobule (A). Centrilobular consolidation (B). Ground-glass opacity (C). Air-space consolidation (D).Fig. 16.10 Air bronchograms. Bronchi are contrasted by the surrounding air-space disease (uremic pneumonia).Fig. 16.11 Ground-glass infiltrate. A hazy pulmonary density is caused by pneumocystic pneumonia.
These densities are observed in conditions in which either air in the acini is only partially replaced by soft tissue-equivalent material or the walls of the acini are diffusely thickened. This appearance is nonspecific and can be found with any early manifestation of a diffuse acinar or interstitial process. Interstitial pneumonias (e.g., viral and pneumocystic [ Pneumocystis carinii, PCP]), desquamative interstitial pneumonitis, and alveolar proteinosis frequently present in this fashion.
Ground-glass opacity (Fig. 16.11) refers to a subtle, hazy increase in lung density on high-resolution CT. It is a nonspecific finding and differs from true air-space disease in that it does not obscure pulmonary vessels. It may likewise result from either alveolar or parenchymal abnormalities. Thus, ground-glass opacities can be caused by intra-alveolar fluid/inflammation, and simply represent an alveolitis, or be affected by mild thickening of the septal or alveolar interstitium (e.g., due to an edema, inflammation, infection or neoplasmatic infiltration). Ground-glass opacities are also often associated with a mosaic pattern, air trapping, “crazy paving,” and fibrosis (e.g., honeycombing). A mosaic pattern simply describes regional differences in parenchymal density due to either air trapping or zones of increased consolidation. Air trapping is highly indicative of an airway disease and appears as normal parenchyma on inspiratory scans and low attenuating regions on expiratory scans. By contrast, zones of increased consolidation remain unaltered during expiratory scans. Crazy paving describes a pattern in which thickened, polygonal interlobular septa are superimposed on ground-glass opacities. This pattern is observed in pulmonary alveolar proteinosis, PCP, acute respiratory distress syndrome (ARDS), hemorrhage, and acute exogenous lipoid pneumonia.
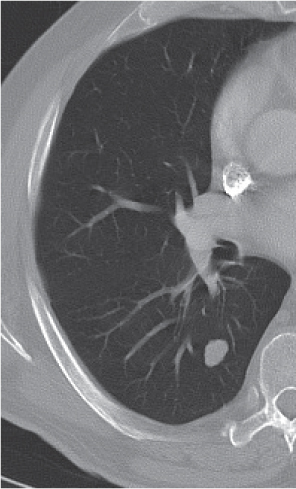
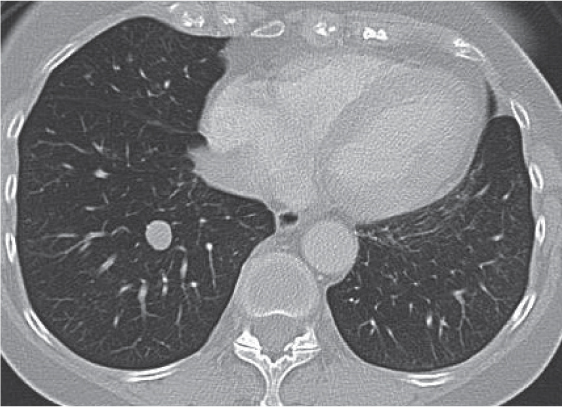
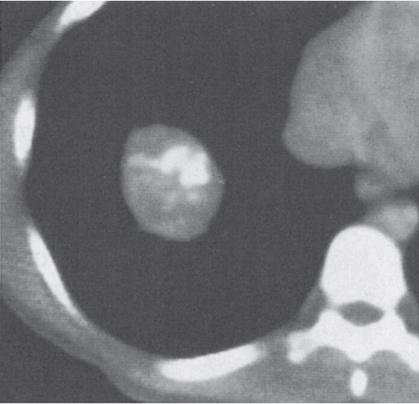
Compared with conventional radiography, pulmonary nodules are detected much earlier and more easily on CT scans. Differentiation between benign and malignant lesions remains a major problem, however. Small peripheral metastases cannot be differentiated from granulomas or intrapulmonary lymph nodes, which are also found in a subpleural location. In case of sepsis or metastatic spread, usually numerous similar-sized pulmonary lesions are found. A vessel entering a small nodule is suggestive of a hematogenous metastasis, but it may also be associated with septic emboli.
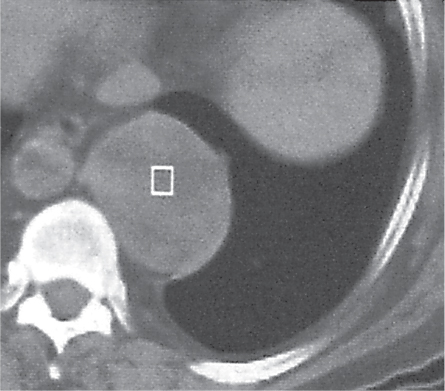
A solitary pulmonary nodule can be assumed benign if it remains stable in volume over a 2-y period. Also, a mean density > 200 HU on noncontrast CT scans is an indicator of a benign lesion. The high attenuation value reflects subtle calcifications within the lesion that are not discernible on the images. In general, visible calcifications are highly suggestive of a benign lesion. Benign calcifications (including histoplasmoma) tend to be either centrally located or diffusely distributed throughout the lesion, whereas eccentric calcifications can also be found in malignant lesions (e.g., scar carcinoma originating from a granuloma or metastases from osteoblastoma). Lack of contrast uptake (< 20 HU increase after bolus injection) is another indicator of a benign lesion. The demonstration of fat within the lesion usually suggests a benign hamartoma or, less commonly, a lipomatous lesion, fat embolus, or lipoid pneumonia. Thus, any solitary nodule with smooth borders measuring < 2 cm in diameter in an a-symptomatic patient younger than 40 y is likely to be benign and should be monitored. Usually a follow-up CT examination within 6 to 9 months and a thorough clinical review and patient history allow further validation.
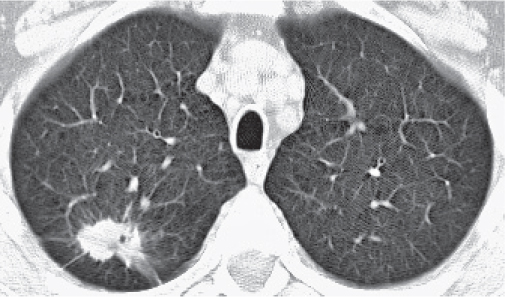
Malignant lesions frequently exceed 2 cm in diameter, have a spiculated margin, and a mean attenuation value < 150 HU on pre-contrast CT scans, as well as eccentric cavitations and, if present, intratumoral calcifications. A bronchovascular bundle converging toward the lesion may be visible, and usually enhancement of the mass is > 20 HU after contrast injection. Additional findings include a notch in the mass, heterogeneity of the lesion, and a surrounding halo of lower density (hemorrhage/lymphangiosis). In a subpleural location, retraction of the pleura toward the mass may produce a pleural tag that is caused by a desmoplastic reaction. All these signs, however, are not specific for a malignancy and may also be found in a variety of benign conditions.
The differential diagnosis of diffuse lung disease is discussed in Table 16.1 and solitary and multiple focal pulmonary lesions in Table 16.2.
Table 16.1 Diffuse lung disease
Disease
CT Findings
Comments
Vascular
Disseminated intravascular coagulation (DIC)
Minimal scattered parenchymal densities to massive pulmonary edema.
Diagnostic pearls: Massive pulmonary edema and the course of the disease often are indistinguishable from those of adult respiratory distress syndrome (ARDS).
Always occurs in the wake of other disorders, such as shock, sepsis, cancer, obstetric complications, burn injuries, and hepatic disease.
Poorly defined consolidations to widespread bilateral air-space opacities often with air bronchograms.
Diagnostic pearls: A coarse reticular pattern may become evident during resolution, which may last between a few days to a week.
Spontaneous pulmonary hemorrhage is associated with several bleeding disorders and vasculitides, such as systemic lupus erythematosus (SLE), polyarteritis nodosa, Henoch–Schönlein purpura, and Wegener granulomatosis.
Minimal to widespread air-space consolidations with predilection for the peripheral zones of the lower lung fields.
On high-resolution CT, bilateral ground-glass opacities and thickening of interlobular septa are seen.
Diagnostic pearls: Micronodular (< 5 mm) centrilobular and subpleural opacities representing alveolar edema or hemorrhage; fat-attenuating pulmonary artery filling defects on contrast-enhanced CT.
Typical complication of (surgery of) long bone fractures.
Onset 1 to 2 days after trauma/surgery. Resolution may take 1 to 4 weeks.
Clinical presentation is classified into major and minor symptoms according to Gurd.
Major criteria comprise subconjunctival/axillary pete-chia, mental changes, hypoxemia, and pulmonary edema. Minor symptoms include fat globuli in sputum or urine, tachycardia, emboli in retina, increasing sedimentation rate, drop in hematocrit or platelet values, and temperatures > 38.5°C (101.3°F). Diagnosis requires at least one major and four minor symptoms.
From smooth thickening of interlobular septa (interstitial edema) via ground-glass opacities in the dependent lung portions (alveolar edema) to (partial) atelectasis of the lung (often with air bronchograms). Pleural effusions are common.
Diagnostic pearls: Changes tend to be more peripheral.
Transudation of fluid into the central and peripheral interstitial space constitutes interstitial edema as the first stage of pulmonary edema. This is followed by transudation of fluid into the air-space (alveolar edema).
With progression, completely opacified acini coalesce, producing a “patchwork quilt” appearance of atelectatic lung portions.
Similar appearance as in cardiogenic edema, but findings tend to be more centrally located.
Diagnostic pearls: “Butterfly wing” congestion of central lung portion.
Noncardiogenic pulmonary edema with elevated microvascular pressure is associated with renal failure (see Fig. 16.10), hypervolemia, hyperinfusion, hypoproteinemia, and neurologic disorders (e.g., head trauma and increased intracranial pressure).
Bilateral patchy to diffuse ground-glass opacities with or without consolidations with air bronchograms; usually more prominent in the perihilar area, as well as middle and lower lung zones (acute phase). Within a few days, ground-glass opacities are replaced by a reticular pattern with smooth septal thickening.
Asymmetric pulmonary fibrosis with coarse reticular pattern and eventually honeycombing is typical for the chronic phase.
Diagnostic pearls: Sparing of costrophrenic angles and subpleural space.
Pleural effusions are unusual.
Rare disease; M > F.
Hemoptysis typically precedes the clinical manifestations of renal disease (glomerulonephritis) by several months.
Hemorrhagic episodes cause bilateral ground-glass opacities, which are soon replaced by interstitial thickening.
Ten to 12 days after onset, interstitial changes typically resolve.
Recurrent bleeding episodes cause progressive interstitial fibrosis. Hilar lymph node enlargement may be observed during acute stage.
Diagnostic pearls: Lack of renal involvement and thus absence of antineutrophil cytoplasmic antibody (ANCA) and antibasal membrane antibodies.
Chronic IPH usually presents with malaise, iron deficiency anemia, finger clubbing, hepatosplenomegaly, and bilirubinemia. Acute IPH is relatively rare and presents with pulmonary hemorrhage and fever.
Diffuse septal thickening through lymphocytic infiltrates and formation of thin-walled cysts with a preference of basal parts of the lung.
Diagnostic pearls:
Diffuse disease:
Classic example for lymphatic distribution pattern of micronoduli (i.e., centrilobular and subpleural micronoduli < 5 mm) within the secondary lobule. “Tree-in-bud” sign not due to bronchiolitis but secondary to thickening of bronchovascular bundles. Thin-walled (1–25 mm) cysts involving < 10% of the lung parenchyma are the most characteristic finding. Associated with diffuse ground-glass opacities/consolidations, septal thickening.
Focal disease:
Air-space consolidations with air bronchograms (pseudolymphoma).
Partly enlarged hilar lymph nodes may initially appear as a focal central mass or simulating central pneumonia.
Usually there are no pleural effusions.
Diffuse disease commonly referred to as LIP, focal disease referred to as pseudolymphoma. Primarily affects middle-aged women.
Histologically, a diffuse hyperplasia of bronchus-associated lymphoid tissue (BALT), which is a subset of mucosa-associated lymphoid tissue (MALT).
LIP is triggered through recurrent antigen exposure, such as viral infections (Epstein–Barr virus, human immunodeficiency virus [HIV], etc.), autoimmune diseases (Sjögren syndrome, rheumatoid arthritis, myasthenia gravis, Hashimoto thyroiditis, etc.), immunodeficiency (graft-vs-host reaction [GvHR]), and drugs.
Treatment depends on stimulating antigen/agent. Lymphatic distribution pattern of micronoduli is also observed in patients with pneumoconiosis, sarcoidosis, lymphangitis carcinomatosa (usually pleural effusions), and amyloidosis.
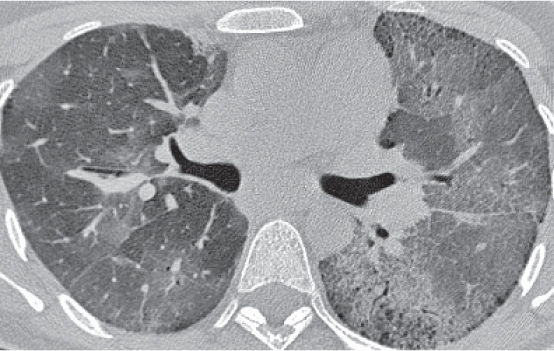
Rapid progressive diffuse alveolar damage of unknown etiology.
Diagnostic pearls: Diffuse bilateral, almost symmetrical ground-glass densities in the lower lung. May develop into architectural distortion and honeycombing with dense air space opacifications with or without bronchiectasis.
Crazy paving is observed.
Rare idiopathic lung fibrosis.
Histological diffuse alveolar damage rapidly progresses through three stages (exudative, proliferative, and fibrotic).
Acute onset of clinical symptoms, which are similar to ARDS or a viral pneumonia.
Interstitial fibrosis with a subpleural and basal preponderance.
Diagnostic pearls: Initially distinct reticular inter-lobular thickening is seen with presence of ground-glass opacifications (thickened interstitium of the secondary pulmonary lobule).
With progression of the disease, a coarse reticulonodular pattern, honeycombing, irregular subpleural thickening, fibrous bands (frequently originating from the pleural surface), traction bronchiectases, and eventually severe architectural distortion.
Often accompanied by centrilobular/paraseptal emphysema.
Histologically, an interstitial inflammation with presence of fibroblasts, lymphocytes, and histiocytes. Typical onset between 40 and 70 y of age, with slight male predominance. Symptoms include progressive dyspnea, nonproductive cough, weight loss, and fatigue. Clinical symptoms include digital clubbing, breathlessness, and noncoughing.
Digital clubbing is common and may precede clinical symptoms.
Moderate progression with overall poor prognosis. Drug reaction may have similar lung patterns and clinical symptoms, which stop immediately after drug abstinence.
May additionally show overlying diffuse interstitial disease (“crazy paving”) that presents initially as a fine reticular pattern and later progresses to a coarser reticulation and, rarely, honeycombing. Fibrotic changes may lead to architectural distortion.
Observed particularly in combination with or as a pulmonary pattern in collagen vascular disease, systemic sclerosis, rheumatoid arthritis, drug-induced pulmonary disease, and hypersensitivity pneumonia, as well as after radiation therapy.
Desquamative interstitial pneumonia (DIP)
Chronic idiopathic interstitial pneumonia often observed in smokers.
Diagnostic pearls: Irregular linear opacities and diffuse ground-glass opacities with a slight preference of the periphery of lower lung zones; some presence of thin-walled small cysts (< 3 cm in diameter).
Honeycombing is unusual.
Histologically, macrophage filling of alveolar spaces. May be the end stage of a chronic respiratory bronchiolitis after having progressed to a respiratory bronchiolitis-associated interstitial lung disease (RB-ILD).
DIP and UIP may reflect different stages of the same disease process.
The clinical course thus can be benign and may completely stop after cessation of smoking with or without steroid treatment.
Multiple small centrilobular nodules and ground-glass opacities with relative sparing of the subpleural space (bronchocentric pattern).
Diagnostic pearls: V- or Y-shaped tubular opacities (“tree-in-bud” sign) and sharply marginated regions of increased lung attenuation (“air trapping”) on expiratory high-resolution CT.
Ground-glass opacities represent centrilobular nodules within secondary lobule.
Spread of disease is bronchogenic.
Involvement of subpleural space is indicative of lymphatic or hematogenous spread (lymphatic pattern).
Bronchiolitis typically associated with toxic smoke/gas inhalation (i.e., respiratory bronchiolitis); viral or mycoplasmatic infections, particularly in children younger than 3 y (infectious bronchiolitis); connective tissue disease (e.g., rheumatoid disease); cryptogenic organizing pneumonia (COP); hypersensitivity pneumonitis; aspiration; pneumoconiosis; and as a late complication after organ transplantation (months to years).
Diagnostic pearls: Subsegmental, segmental, or lobular atelectasis with right upper lobe predilection and recurrent focal pneumonitis (air-trapping, tree-in-bud sign, mosaic perfusion).
Prominent hili may be caused by a combination of peribronchial cuffing, mild adenopathy, and enlarged pulmonary arteries (secondary pulmonary hypertension).
Autosomal recessive disease with 1:2000 incidence, almost exclusively observed in Caucasians.
Positive sweat test (abnormally high chloride concentrations) is diagnostic.
Peribronchial thickening and prolonged mucous plugging result in hyperinflation with subsequent development of bullae and both tubular and cystic bronchiectases.
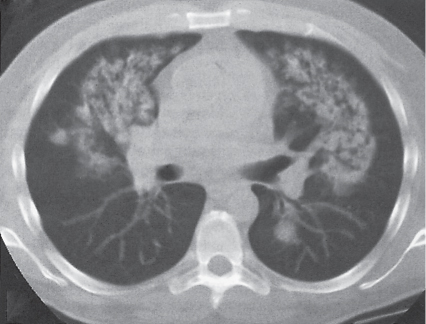
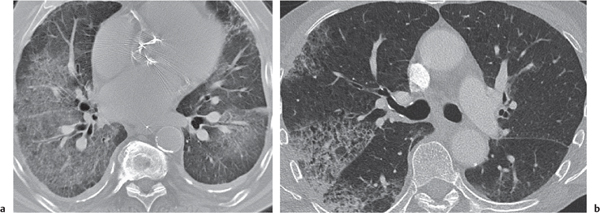
Micronodular (1–10 mm) thickening of the interstitium predominantly affecting the middle and upper portions of the lung.
Diagnostic pearls: Typical features are thickened interlobular septa, subpleural lines and nodular pleural irregularities, radiating fibrous bands, honeycombing, and traction bronchiectases.
In 10% of cases, nodules may calcify centrally (especially in silicosis). Hilar adenopathy is frequently present and may in 5% of cases show calcifications in a characteristic “eggshell” pattern (especially in silicosis).
Nodules may aggregate into progressive massive fibrosis (PMF), presenting as bilateral dense opacities most often observed in the dorsal aspect of the upper lobes.
PMF may cavitate.
Silica is more fibrogenic than coal.
Silica/coal particles are inhaled into respiratory bronchioles and subsequently digested by macrophages and lymphocytes. These macrophages transport the particles to hilar and mediastinal lymph nodes, forming granulomas.
It usually takes 10 to 20 y of exposure before radiologic abnormalities become evident.
However, acute silicosis of sandblasters may present in < 1 y as diffuse air-space disease.
Caplan syndrome: rheumatoid arthritis associated with pneumoconiosis, especially coal workers’ pneumoconiosis.
Peripheral interstitial fibrosis usually located in lower parts of the lung and presenting with thickened interlobular septa, centrilobular nodules, curvilinear subpleural lines, fibrous bands, and honeycombing.
Diagnostic pearls: Nodular pulmonary pattern and hilar adenopathy are unusual and not characteristic. May be associated with asbestos-related pleural disease, round atelectasis, pulmonary or interlobular fissural fibrous masses, bronchogenic carcinoma, and mesothelioma.
A round atelectasis is a round or lentiform subpleural density with a “comet tail” produced by the curvilinear bronchovascular bundle entering the lesion.
Asbestos fibers are very thin, heat resistant, and durable. After inhalation, they travel into lower lung zones and are deposited into respiratory bronchioles. They are too large to be removed by lymphocytes or macrophages and thus lead to a distinct local fibrosis. Pleural disease usually is induced after penetration of these fibers through the lung into the pleural space. Asbestos-related pleural disease consists of focal pleural plaques (70%), diffuse pleural thickening (20%), pleural calcifications (20%), and pleural effusions (20%).
Talcosis resembles asbestosis and asbestos-related pleural disease.
Aluminium (bauxite) pneumoconiosis: Coarse reticulonodular pattern often associated with pleural thickening.
Berylliosis
Sarcoidosis-like lung pattern in patients with exposure to beryllium (nuclear power plants, electronic/aerospace industries).
Diagnostic pearls: Nodular to reticulonodular pattern sparing apices and bases, sometimes associated with hilar and mediastinal adenopathy. Pulmonary nodules may calcify (differential diagnosis: sarcoidosis).
Probably a type IV hypersensitivity reaction to beryllium dust.
Acute berylliosis is rare and presents as pulmonary edema following an overwhelming exposure.
Radiopaque dust inhalation (iron, tin, barium, antimony, and rare-earth compounds)
Dense granular stippling uniformly distributed over both lung fields.
Diagnostic pearls: Density of the tiny nodules correlates with the atomic number of the inhaled element.
Usually lack of clinical symptoms, as these substances are not fibrogenic.
In mixed dust disease (e.g., in association with silica) pulmonary granulomas and fibrosis may occur (e.g., siderosilicosis).
Silo filler’s disease (NO2 inhalation)
Acute bronchiolitis with bilateral reticulonodular or patchy infiltrates in the middle and lower lung fields that may progress rapidly to massive air-space disease within 24 hours.
Diagnostic pearls: Complete resolution typically occurs within a few days if not fatal. After 2 to 5 weeks, bronchiolitis obliterans develops with multiple discrete nodular opacities of varying size scattered throughout both lung fields.
NO2 inhalation injuries may also be associated with industrial exposure to fuming nitric acid or the use of explosives in mining operations.
Exposure to other toxic gases such as SO2, H2S, ammonia, chlorine, and phosgene causes similar pulmonary abnormalities.
Bilateral peripheral air-space disease, occasionally with ground-glass appearance and mildly thickened interlobular septa.
Diagnostic pearls: Thickened interstitium affects polygonal opacities with central ground-glass appearance (crazy paving). Also seen: geographic distribution of ground-glass opacities on high-resolution CT. A coarse reticular pattern simulating honeycombing is less common. Pleural effusions are absent.
Age peak: 20 to 50 y.
Often observed in immunocompromised patients.
M > F (3:1). Fungal infections such as from Nocardia, Aspergillus, and Cryptococcus are typical and often associated.
Alveolar microlithiasis
Bilateral atypical dense appearance of lung.
Diagnostic pearls: Superimposition and summation of discrete and extremely sharply defined microliths measuring < 1 mm in diameter.
On high-resolution CT, characteristically micronodular calcifications are superimposed on ground-glass opacities.
Rare disorders of obscure etiology with familial occurrence in over 50% of cases.
Typically without clinical symptoms.
Usually found in patients between 30 and 50 y of age but may also be observed in infants.
May eventually result in cardiac/lung failure.
Smoke and fume inhalation
Bilateral patchy parenchymal densities (transient pulmonary edema) developing within hours after exposure.
Diagnostic pearls: Patchy lung densities may resolve within a few days or progress to severe pulmonary air-space disease with atelectasis, hemorrhage, necrosis, and pneumonia.
May eventually result in ARDS.
Characteristic pulmonary parenchymal disease in patients with burn injuries.
May be caused by three mechanisms: toxic combustion products, direct trauma from heat, and shock and sepsis.
Allergic lung disease caused by a variety of organic and chemical antigens.
Diagnostic pearls: Always compare inspiratory with expiratory high-resolution CT.
Acute stage: Bilateral air-space consolidations and ill-defined centrilobular micronodules, predominantly affecting the middle and lower portions of the lung. Subacute stage: Patchy ground-glass opacities, illdefined centrilobular micronodules, mosaic perfusion (air trapping), and cyst formation (middle and lower portions of the lung).
Chronic stage: Diffuse interstitial fibrosis characterized by a coarse reticular pattern, honeycombing architectural distortion, and formation of traction bronchiectases.
Often associated with loss of volume, especially in the upper lobes, and compensatory inflation of the least-affected lung zones.
Typically sparing of costophrenic angles.
Acute or insidious onset of progressive dyspnea.
Radiographic findings usually parallel clinical symptoms but are also observed in symptom-free patients.
Both type III (immune complex) and type IV (cell-mediated) reactions are regarded as inducing mechanisms. Sources of exposure include moldy hay (farmer’s lung), pigeons, canaries, parakeets, chickens (bird fancier’s lung), moldy sugar cane residuals (bagassosis), moldy cheese (cheese washer’s lung), air conditioning, humidifiers, damp walls or floors, and hot tubs (humidifier lung). Treatment of choice is avoidance of antigen exposure and steroids (during the acute stage).
A heterogeneous pattern of air-space and interstitial changes in patients with long-lasting exposure to a variety of drugs.
Diagnostic pearls: Lung manifestations range from pulmonary edema (e.g., heroin, intravenous [IV] contrast agents, salicylates) and patchy air-space disease (e.g., amiodarone, chlorpromazine) to an interstitial disease of a reticular or reticulonodular nature (e.g., chemotherapeutic agents, nitrofurantoin) that may progress to honeycombing (see also Fig. 16.19).
The time span for development and resolution of pulmonary changes depends on the mechanism involved and thus is extremely variable, ranging from a few hours to several months.
Pulmonary disease is caused by drug hypersensitivity or toxicity.
Typical concomitant clinical manifestations are spasmodic asthma, noncardiogenic edema, Löffler syndrome, interstitial and alveolar pneumonitis, SLE-like syndromes, and pulmonary vasculitis.
Diffuse interstitial pneumonitis and fibrosis presenting as reticulonodular to coarse reticular pattern and honeycombing with more frequent involvement of the lower lung fields.
Diagnostic pearls: COP-like pattern, mosaic perfusion with air trapping on expiratory high-resolution CT, and bronchocentric pattern of nodules (granulomas) (see also Figs. 16.18,16.19).
Nodules range from 5 mm to 5 cm in diameter and may cavitate.
Large nodules often are found in a subpleural location, may be lobulated, and resemble neoplasms. Concomitant pleuritis and fibrobullous changes in the upper lobes are other rare manifestations.
More common in middle-aged women with rheumatoid arthritis. Complications such as superimposed infections, amyloidosis, and respiratory failure may lead to death.
Unilateral or bilateral pleural effusion is the most frequent manifestation of rheumatoid disease in the thorax. In the majority of cases, it is the sole thoracic abnormality and precedes other lung abnormalities. These pleural abnormalities may help to differ rheumatoid arthritis–related lung disease from usual interstitial pneumonia (UIP).
Treatment of choice is classic rheumatoid arthritis medication.
Pulmonary scleroderma
Generalized connective tissue disease affecting several organ systems, including the gastrointestinal (GI) tract, lung, skin, heart, and kidneys.
Diagnostic pearls: Nonspecific interstitial pneumonitis (NSIP) with ground-glass opacifications and diffuse interstitial disease, presenting initially as a fine reticular pattern, progressing to coarser reticulation and rarely, honeycombing. Changes particularly affect lower lung zones. Progressive loss of lung volume with worsening of the disease.
Absent pleural reactions characteristic (see Figs. 16.18,16.19).
Histologically, an overproduction and tissue deposition of collagen.
Particularly affects middle-aged (30–50 y) women. Pulmonary findings may resemble idiopathic pulmonary fibrosis. An air-filled dilated esophagus due to aperistalsis and/or soft tissue calcinosis (e.g., around the shoulders) may be associated and is pathognomonic.
Discrete bilateral pleural effusions/pleural thickening in young female patients with a history of SLE.
Diagnostic pearls: Pleural and pericardial effusions; bilateral subpleural reticular opacities with or without honeycombing; bronchocentric micronodular pattern (tree-in-bud); bronchiectasis/bronchial wall cuffing; lupus pneumonitis with coarse linear bands and patchy ground-glass opacities in the periphery of the lung. Seldom edema or hemorrhage (see also Fig. 16.19).
Radiographic manifestations of drug-induced and idiopathic SLE are identical.
Interstitial lung manifestations similar to scleroderma, but less frequent and less severe. Pathologic changes typically resemble NSIP, COP, or UIP, or a combination of the three.
Diagnostic pearls: Patchy symmetric bilateral subpleural consolidations in combination with reduced lung volumes; bilateral symmetric basal ground-glass opacities; reticular opacities with coarse parenchymal bands and irregular thickening of the bronchovascular bundle. May finally result in honeycombing and architectural distortion (see also Figs. 16.18,16.19).
Rare autoimmune disease affecting particularly middle-aged women (twice as often as men). Paralysis of pharyngeal and respiratory muscles may result in aspiration and diaphragmatic elevation, respectively.
Bilateral symmetric basal ground-glass opacities are a sign of an ongoing, active inflammation process. Steroids are treatment of choice.
Bilateral basal linear densities may be residual findings after steroid treatment.
Sjögren syndrome
Interstitial disease of reticulonodular nature and patchy infiltrates, sometimes associated with small effusions.
Diagnostic pearls: Similar findings as observed in diffuse LIP: centrilobular and subpleural micronoduli (lymphatic pattern), thin-walled (1–25 mm) cysts, bronchiolitis (tree-in-bud sign), and diffuse ground-glass opacities or consolidations (see Fig 16.16).
Particularly affects middle-aged women.
Occurs in 90% of patients presenting with sicca syndrome (i.e., keratoconjunctivitis sicca, xerostomia, and recurrent parotid gland swelling). Secondary Sjögren syndrome is associated with rheumatoid arthritis and other connective tissue diseases, transplant recipients, and acquired immunodeficiency syndrome (AIDS).
Diagnostic pearls: Irregular consolidations in predominantly subpleural location, randomly distributed ground-glass opacities, and nodules. Consolidations appear to ignore lobular structure of the lung.
Typically affects middle and lower portions of the lung.
Idiopathic alveolar disease extends into small airways. Contrary to macroscopic appearance, lung architecture is preserved (no fibrosis). Histologically, chronic inflammatory and fibroblastic tissue.
Clinical symptoms are chronic cough, dyspnea, and fever over a 3- to 6-month period prior to diagnosis. Important differential diagnosis to pneumonia, lymphoma, and sarcoidosis.
Diffuse bilateral reticular pattern with upper and mid-zone predominance and consisting of multiple small irregular nodules and small cysts embedded within normal lung parenchyma.
Diagnostic pearls: Centrilobular, peribronchial nodules (1–5 mm in diameter).
Larger nodules may occasionally exceed 10 mm and cavitate.
Thin-walled cysts (< 10 mm), equally distributed through the central and peripheral lung zones. Pulmonary fibrosis with interlobular septal thickening, honeycombing, and enlarging cystic spaces (up to several centimeters in diameter) may become evident with progression of the disease. Hilar adenopathy and pleural effusions are unusual in adults.
Occurs usually in middle-aged Caucasian patients, typically with a history of nicotine abuse. Histologically, a diffuse destruction of distal airways induced by granulomas containing large mononuclear cells with characteristic cytoplasmic inclusions (Langerhans cells).
At the time of diagnosis, ~25% of patients are asymptomatic. Nonproductive cough is the most common presentation in the remaining patients. Spontaneous pneumothorax is a frequent complication in advanced stages.
Disease may regress, resolve completely, stabilize, or progress to advanced fibrosis.
Treatment includes smoking cessation and steroids. Severe forms may require lung transplantation.
Symmetric mediastinal and hilar lymphadenopathy with or without micronodular lung opacities, involving preferentially the middle and upper portions of the lung.
Diagnostic pearls:
Interstitial pattern (common): In early stages, multiple micronoduli (< 5 mm) with perivascular, centrilobular, perilymphatic (i.e., along bronchovascular bundles) distribution.
In advanced stages, a coarse reticulonodular pattern with thickened interlobular septa. Nodules > 1 cm in diameter are rare, and cavitation is unusual. Progression of the disease results in fibrosis with honeycombing, long linear bands extending to the pleural surface, cicatricial bronchiectases, progressive massive fibrosis, and large bullae (up to 10 cm). “Alveolar” pattern (uncommon): Indistinctly defined peripheral densities, sometimes with ground-glass appearance, resembling an active alveolitis.
Coalescence of these densities produces large opacities, often with air bronchograms, located either centrally or peripherally in the lung.
Highest incidence in black women between 20 and 40 y of age. Approximately half of patients are asymptomatic at time of diagnosis.
Histologically, well-defined granulomas with a rim consisting of fibroblasts and lymphocytes.
Hilar and mediastinal (azygos and aortopulmonic window) adenopathy is by far the most common intrathoracic manifestation (80%).
Progressive cystic destruction of the lung induced by proliferating atypical muscle cells.
Diagnostic pearls: Well-defined, uniformly thin-walled cysts distributed diffusely throughout both lungs, slightly prominent at the lung bases, as well as scattered ground-glass opacities. Cysts enlarge and coalesce (up to several centimeters in diameter) with progression of the disease.
Rare disease, exclusively found in women of child-bearing age.
May be a forme fruste of tuberous sclerosis that can present with identical pulmonary CT findings. Mediastinal lymphadenopathy, chylous pleural with or without pericardial effusions, and recurrent pneumothorax are common associated findings.
Radiation pneumonitis is observed during acute stage, radiation fibrosis during chronic stage.
Diagnostic pearls: Pulmonary findings are strictly confined to the radiated area of the lung.
Radiation pneumonitis: Ground-glass opacities, patchy consolidations often with air bronchograms, and occasionally loss of volume (due to loss of surfactant or bronchiolar plugging).
Radiation fibrosis: Severe shrinkage of the radiated lung, fibrous bands, traction bronchiectasis, solid consolidations (fibrosis) with spiculated borders, and localized pleural thickening.
Radiation damage to the lung increases with the dose and is lessened by fractionation.
Pulmonary changes are not observed for a fractionated dose of < 3000 rads.
Pulmonary manifestations may occur at any time within the first 6 months after cessation of the radiotherapy.
Though delayed changes are common, any pulmonary changes occurring > 1 y after radiotherapy are highly unlikely to be caused by the radiotheraphy.
Parenchymal changes due to a thromboembolic disease of the pulmonary arteries.
Diagnostic pearls: CT density of the lung distal to occluded arteries may be either decreased (oligemia or Westermark sign) or increased (atelectasis, edema, or hemorrhage). Peripheral wedge-shaped areas of consolidation with neither air bronchograms nor cavitation represent either atelectasis or infarcts, the latter corresponding to a Hampton hump on conventional radiographs. Small pleural effusions are common.
Dyspnea, pleuritic chest, and deep vein thrombosis are a common clinical presentation. Laboratory findings include electrocardiogram (ECG) changes and abnormal blood gas levels.
Septic emboli present as multiple, ill-defined, round or wedge-shaped opacities with frequent cavitation in the lung periphery. Predisposing factors are IV drug abuse, immune deficiency, IV catheters, alcoholism, and congenital heart disease.
Predominantly trauma-induced contusion of lung parenchyma.
Diagnostic pearls: Irregular patchy air-space opacities to diffuse consolidations and discrete pleural effusions.
Rib fractures may be absent.
Parenchymal contusion zones appear within 6 hours after injury (usually blunt chest trauma) and resolve within 3 days. They consist of edema and blood in the absence of substantial tissue disruption.
Aspiration of solid or fluid material into large airways.
Diagnostic pearls: Patchy infiltrates to homogeneous consolidations; usually symmetric bilateral gravitational distribution, which may also be asymmetric (depending on position of patient at time of aspiration) and segmental to lobular atelectasis. Superinfection may lead to necrotizing pneumonia with abscess formation and central cavitation.
Chronic aspiration pneumonia is associated with Zenker diverticulum, esophageal stenosis, achalasia, tracheoesophageal fistula, and neuromuscular disorders involving the pharynx. May eventually lead to residual scarring of lung parenchyma.
Lung changes in nonchronic aspiration usually resolve within 7 to 10 days after proper treatment (steroids and antibiotics).
Aspiration of amniotic fluid
Diffuse ubiquitous pulmonary consolidations, often rapidly increasing in size and density with lethal outcome.
Affects exclusively neonates at birth. Predisposing factors include difficult labor, intrauterine fetal death, advanced maternal age, and multiparity.
Aspiration due to near drowning
Symmetrical widespread pulmonary edema that may occasionally be delayed up to 2 days.
Edema usually resolves completely within 3 to 5 days, but may also last up to 10 days.
Focal parenchymal consolidation in patients with fever.
Diagnostic pearls: Focal patchy air-space consolidations, often associated with areas of consolidations and air bronchograms. Discrete pleural effusions, atelectasis, and cavitation are common.
On contrast-enhanced CT, differential diagnosis to simple compression atelectasis is possible due to a lack of contrast media uptake in pneumonic parenchyma.
Bronchogenic; usually spread by inhalation (e.g., Staphylococcus), aspiration (anaerobics), or direct invasion (i.e., abscesses, cavities; e.g., in tuberculosis [TB]).
Hematogenous spread usually through anaerobics (e.g., Pseudomonas).
Old compression atelectasis may not show contrast media uptake due to the Euler–Liljestrand mechanism.
Most commonly, pneumonia due to an infection with mycobacteria TB.
Diagnostic pearls: In primary TB localized micronodular airspace opacities usually confined to one lobe in the upper part of the lung.
May in advanced stages spread bronchogenically to other lobes and thus lead to numerous bronchocentric air-space consolidations (tree-in-bud sign).
Often concomitant hilar and/or mediastinal adenopathy.
In secondary or miliary TB, hematogenous spread and thus lymphatic distribution pattern of uniform micronodules (involving the subpleural space). Pleural effusions are common.
Usually secondary to mycobacteria TB.
In rare cases, pneumonia may be due to Mycobacterium avium infection (MAI). A pathognomonic pattern in these patients is the presence of widespread centrilobular micronodules in combination with ventral bronchiectasis in the middle lobe with or without lingula.
Lymphatic pattern in miliary TB is due to hematogenic seeding.
Pneumonia, viral and mycoplasma
Diffuse interstitial thickening in patients with fever.
Diagnostic pearls: Variable appearance depending on virus type. Typical is interstitial thickening with or without presence of centrilobular nodules. Ground-glass opacities usually only superimposed in advanced stages.
Most common in children and young adults. Signs of myoplasma pneumonia are usually not discernible from those of viral pneumonia.
Diffuse interstitial thickening in immunocompromised patients with fever.
Diagnostic pearls: Thickened interlobular septa and centrilobular micronodules, usually involving lung periphery, and diffuse ground-glass opacities (less prominent than in pneumocystic pneumonia). Small pleural effusions are frequently associated.
Particularly affects neonates and immunocompromised patients (especially organ transplant recipients).
Diffuse ground-glass opacities predominant findings in Hantavirus and severe acute respiratory syndrome (SARS).
Lobular ground-glass opacities also observed in herpes simplex and influenza.
Segmental consolidations observed in adenovirus.
Pneumonia, fungal
Discrete air-space consolidations in immunocompromised patients with fever.
Diagnostic pearls: Patchy, homogeneous, poorly defined peribronchial ground-glass opacities with or without centrilobular nodular pattern.
Disseminated disease is an early appearance of acute fungal sepsis and is found particularly in immunocompromised patients. Patients may still be symptom-free.
Focal consolidations and cavitations are much more typical for fungal infections but are typically observed only in subsequent stages.
The most common fungi are Candida and Aspergillus.
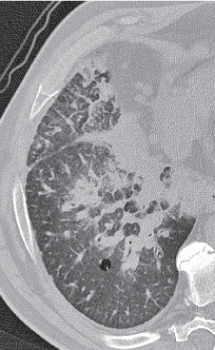
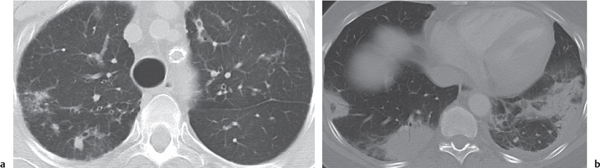
Diagnostic pearls: Bilateral ground-glass opacities with sparing of the subpleural space are the dominant finding. Also characteristic are superimposed intra- and interlobular septal thickening leading to crazy paving, lack of tree-in-bud sign, often mosaic pattern caused by alternating involvement and sparing of subsegmental areas.
Thin-walled cysts are frequently associated, especially in the upper lobes, and may lead to spontaneous pneumothorax.
Pleural effusions and hilar adenopathy are not characteristic.
May evolve into asymmetric consolidations and reticular opacities if not treated.
In immunocompromised patients, particularly those with AIDS, pneumocystic pneumonia is the most frequent pulmonary complication.
Presents with an abrupt onset of dyspnea, hypoxemia, and nonproductive cough. Diagnosis is made with bronchoalveolar lavage in > 90% of cases. Symptoms in AIDS patients usually subacute, developing within weeks.
Symptoms in non-HIV patients usually rapid, evolving over 5 to 10 days.
Cysts are observed only in HIV-associated pneumocystic pneumonia.
Diagnostic pearls: Ground-glass opacities (interstitial and alveolar edema and hemorrhagic fluid) and dense parenchymal consolidations (atelectasis) in the dependent lung in combination with normally aerated lung.
Can be differentiated from cardiogenic pulmonary edema by a normal heart size, more diffuse lung involvement, extensive and conspicuous air broncho-grams, a cystic or “bubbly” appearance of the parenchymal involvement after 7 days, and the absence of significant pleural effusion.
ARDS is defined as noncardiogenic pulmonary edema with normal microvascular pressure and increased capillary permeability. It may be due to direct injury to the lung (i.e., primary or pulmonary ARDS) or capillary leakage (i.e., indirect or extrapulmonary ARDS). ARDS may occur secondary to trauma, shock, sepsis, aspiration, and a variety of other direct or indirect pulmonary insults.
In premature infants, a “spongy” lung pattern is associated with bronchopulmonary dysplasia due to prolonged high oxygen therapy.
Clearly demarcated cavities in the centrilobular portion of the secondary pulmonary lobule.
Diagnostic pearls: Primarily affects upper portions of lung zones (apex, apica segment of lower lobules). Margins of the secondary pulmonary lobule are preserved.
Emphysematous cavities lack a wall and are surrounded by normal lung parenchyma.
Histologically, an enlargement and destruction of alveolar walls. Strongly associated with nicotine abuse; also observed after inhalation of industrial dust. Slight male predominance; peak age between 40 and 75 y.
Smoking abstinence may stabilize or slow down the disease.
More severe cases require medical therapy (bronchodilators) or surgery (lung volume reduction/lung transplantation).
Ill-defined diminishing of lung parenchyma without fibrosis.
Diagnostic pearls: Homogeneously distributed diminishment of the interstitium due to acinar enlargement without zonal preference. Differentiation of normal and diseased lung often difficult.
Lung with a threshold HU density < −960 is emphysematous.
Histologically, destruction of alveolar tissue with abnormal enlargement of all parts of the acinus. Commonly associated with alpha-1-antitrypsin deficiency.
Slight male predominance. Only symptomatic in patients with advanced disease.
No therapy may be necessary, but severe cases may require surgical lung volume reduction or even lung transplantation.
AIDS-associated bilateral pulmonary neoplasm with concomitant involvement of skin, lymph nodes, and GI tract.
Diagnostic pearls: Bilateral ill-defined noduli and coarse reticulonodular opacities with basilar preference, as well as thickening of the bronchovascular bundle with ill-defined perihilar consolidations.
Abnormal endothelial vascular channels embedded within spindle-shaped stromal cells.
Herpes virus associated disease; > 90% occur in male AIDS patients with low CD4 count and concomitant skin and/or mouth lesions. Hilar adenopathy and pleural effusions are associated in ~25% of cases.
Pneumonia-like progressive regional/lobular consolidation of the lung.
Diagnostic pearls: Uni- to bilateral focal or multifocal air-space opacities; increased volume of affected lobe (no atelectasis); ill-defined lobulated and/or spiculated peripheral nodules; ground-glass-opacities with or without reticulonodular pattern (crazy paving). After contrast administration, vessels typically opacify within consolidations (CT angiogram sign). Pleural effusions and local lymph node involvement are uncommon.
Histologically, cancer arising from bronchiolar epithelium and type II pneumocytes.
Cancer cells typically spread bronchogenically via the tracheobronchial tree (cancer pneumonia).
Any antibiotic-resistant pneumonia-like consolidation is highly suspicious.
Local form presenting as a well-circumscribed peripheral mass is more common. Diffuse form presenting as bilateral chronic consolidations with air bronchograms is rare. Overall poor prognosis.
Diagnostic pearls: Typically ill-defined consolidations with air bronchograms (nodules ranging from diffuse miliary pattern to only a few large lesions); coarse perihilar reticulonodular pattern (caused by direct extension from hilar lymph nodes); and peripheral interstitial disease with irregular thickened subpleural lines, interlobular septa, and lymphatic nodular distribution pattern (centrilobular nodules involving the subpleural space) (see also Fig. 16.19, p. 601).
Lung infection in patients with lymphoma is more often due to drug reactions, concomitant pneumonia, or hemorrhage rather than the underlying disease itself.
Pulmonary manifestation of lymphoma is usually associated with or subsequent to hilar and mediastinal lymph node involvement.
Similar pulmonary manifestations may be observed in patients with leukemia.
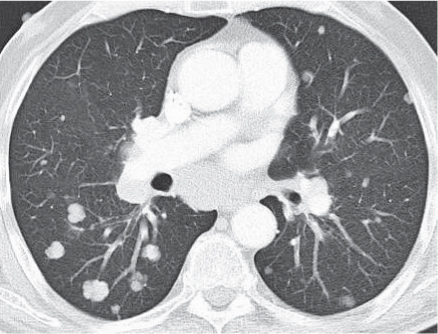
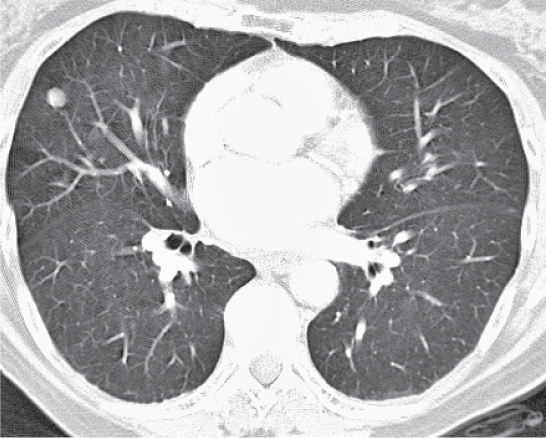
Pulmonary involvement due to lymphatic or hemorrhagic spread of neoplasm.
Diagnostic pearls: Classic lymphatic nodular distribution pattern (i.e., clusters of similar-sized centrilobular nodules, which are diffusely distributed throughout the entire lung and involving also the subpleural space). Arterial feeders entering single lesions are common but not specific (differential diagnosis: septic emboli and other hematogenous infections).
Nodular pulmonary metastases are commonly associated with neoplasms of the lung, kidney, colon, gonads, uterus, bone, head, and neck (including thyroid), melanomas, and soft tissue sarcomas.
An important differential diagnosis is pulmonary septicemia, which may not be discernible from hematogenous spread of metastases on imaging findings alone.
Diagnostic pearls: Usually asymmetric nodular septal thickening confined to one lung/lobe (may also involve both lungs; may resemble edema: Kerley B lines on radiographs); centrilobular micronodules involving the subpleural space (lymphatic distribution pattern); nonspecific patchy ground-glass opacities with or without septal thickening (crazy paving). Pleural effusions and associated hilar/mediastinal lymph nodes are common.
Typical clinical syndrome is shortness of breath. Commonly observed in breast, prostate, stomach, pancreas, and lung cancer.
Poor prognosis.
Fig. 16.12 Diffuse alveolar hemorrhage. Widespread bilateral air-space opacities.Fig. 16.13 Pulmonary fat embolism. Discrete form with bilateral ground-glass opacities in a subpleural location.Fig. 16.14 Cardiogenic pulmonary edema. Smooth thickening of interlobular septa, along with ground-glass opacities, in the dependent lung portions and air bronchograms. Bilateral pleural effusion.Fig. 16.15 Goodpasture syndrome. Bilateral dense air-space consolidations are visible, sparing the lung periphery (butterfly distribution).Fig. 16.16 Lymphocytic interstitial pneumonia. Focal disease (pseudolymphoma) of the right lung, simulating pneumonia. Also visible are diffuse ground-glass opacities, loose subpleural centrilobular micronoduli, septal thickening, and formation of a thin-walled cyst. Note the absence of pleural effusions. Sjögren syndrome would present with bilateral rather than focal disease.Fig. 16.17 Acute interstitial pneumonia. Diffuse bilateral ground-glass opacities. Note the marked “crazy paving” and signs of architectural distortion, including honeycombing and dense air-space opacifications, particularly affecting the left lung.Fig. 16.18a, b Idiopathic pulmonary fibrosis. Initially distinct reticular interlobular thickening with the presence of ground-glass opacifications (a). End-stage disease with a coarse reticulonodular pattern, honeycombing, irregular subpleural thickening, fibrous bands (frequently originating from the pleural surface), traction bronchiectases, and accompanying centrilobular emphysema (b).Fig. 16.19a, b Nonspecific interstitial pneumonia (NSIP). Initially ill-defined bilateral patchy ground-glass opacifications (a), progressing in later stages to a coarser reticulation (b). This pattern is also observed in collagen vascular diseases, rheumatoid arthritis, drug-induced pulmonary disease, and hypersensitivity pneumonia, as well as after radiation therapy.Fig. 16.20 Bronchiolitis. Multiple small V- and Y-shaped centrilobular opacities (“tree-in-bud” sign) and ground-glass opacities with relative sparing of the subpleural space (bronchocentric pattern), as well as implied regions of air trapping.Fig. 16.21a, b Cystic fibrosis. Varicose bronchiectasis with peribronchial cuffing and mucous plugging, particularly affecting the middle lobe of the right lung (a). Advanced disease with architectural distortion and extensive chronic pulmonary infiltrates (b).Fig. 16.22 Silicosis. Multiple well-defined nodules with middle and upper lung zone predominance.Fig. 16.23 Pulmonary asbestosis. Peripheral coarse interstitial thickening mostly involving the lower lung zones.Fig. 16.24 Round atelectasis in pulmonary asbestosis. A subpleural mass with three irregular bands radiating from the mass into the lung parenchyma (crow’s feet) is visible in the right posterior chest. Note the bilateral peripheral interstitial thickening as an early sign of pulmonary asbestosis.Fig. 16.25 Pulmonary alveolar proteinosis. Bilateral peripheral air-space disease with ground-glass appearance and mildly thickened interlobular septa (“crazy paving”). The pleural effusion on the left is uncommon.Fig. 16.26a–c Extrinsic allergic alveolitis. Acute stage with bilateral air-space consolidations and ill-defined centrilobular micronodules (a). Subacute stage with patchy ground-glass opacities, ill-defined centrilobular micronodules, and air-trapping (b). Chronic stage with a coarse reticular pattern, honeycombing, architectural distortion, and formation of traction bronchiectases (c).Fig. 16.27a, b Drug-induced pulmonary disease. Distinct ground-glass opacities (a) with an overlying reticular pattern due to amiodarone. Reticulonodular pattern with patchy subpleural air-space opacifications (b) that partly progress to honeycombing due to methotrexate.Fig. 16.28 Rheumatoid lung. Nonspecific septal thickening and honeycombing in the middle lobe of the right lung. A singular, slightly lobulated nodule apical is seen in the right lower lobe.Fig. 16.29 Systemic lupus erythematosus. Pleural effusions and dominant pneumonitis with poorly defined patchy air-space opacities involving predominantly the periphery of both lower lobes.Fig. 16.30a, b Cryptogenic organizing pneumonia (COP). Randomly distributed ground-glass opacities and nodules (a) that soon progress to irregular consolidations in a predominantly subpleural location that apparently ignores the lobular structure of the lung (b).Fig. 16.31a, b Histiocytosis X. Diffuse bilateral irregular nodules (a) that cavitate and become thick-walled cysts. In the end, patients present with numerous thin-walled cysts (> 10 mm), which are equally distributed throughout the lung (b).Fig. 16.32a–c Pulmonary sarcoidosis. Symmetric mediastinal lymphadenopathy (a) with perilymphatic (i.e., along bronchovascular bundles) micronodular lung opacities involving the upper portion of the right lung (b). Progression of the disease results in progressive massive fibrosis (c).Fig. 16.33 Lymphangioleiomyomatosis. Multiple well-defined, uniformly thin-walled cysts distributed diffusely throughout both lungs.Fig. 16.34 Radiation-induced lung disease. Paramediastinal fibrosis restricted to those parts of the lung that had been irradiated (due to a mediastinal lymphoma).Fig. 16.35a, b Thromboembolic pulmonary disease. Large thrombus within the right pulmonary artery with a peripheral wedge-shaped area of consolidation representing infarcted lung.Fig. 16.36 Pulmonary contusion. Trauma- induced dorsal contusion of both lungs with irregular patchy air-space opacities, discrete pleural effusions, and ventral pneumothorax on the left side.Fig. 16.37 Aspiration pneumonia. Symmetric bilateral segmental atelectasis with air bronchograms and discrete ground-glass opacities.Fig. 16.38 Bacterial pneumonia. Patchy air-space consolidations in the apical left lower lobe.Fig. 16.39 Mycobacterial pneumonia. Miliary tuberculosis (TB) with a lymphatic distribution pattern (involvement of the subpleural space) of multiple equally sized micronoduli.Fig. 16.40 Cytomegalovirus. Thickened interlobular septa and centrilobular micronodules, particularly involving the lung periphery. Also note the concomitant diffuse ground-glass opacities.Fig. 16.41a, b Pneumocystis pneumonia. Acute stage showing bilateral ground-glass opacities with sparing of the subpleural space (a). A 4-month follow-up examination in the same patient without treatment shows progression into asymmetric reticular consolidations (b).Fig. 16.42a, b Centrilobular emphysema. Clearly demarcated pulmonary cavities surrounded by normal lung parenchyma (a), which primarily affects the upper portions of lung zones (b).Fig. 16.43a, b Panlobular emphysema. Homogeneously distributed diminishment of the interstitium (a), resulting in bullous emphysema (b).Fig. 16.44a, b Pulmonary Kaposi sarcoma. Bilateral ill-defined noduli and coarse reticulonodular opacities with basilar preference (a). Another patient with thickening of the bronchovascular bundle and ill-defined perihilar consolidations (b).Fig. 16.45a, b Alveolar cell (bronchoalveolar) carcinoma. Examples of unilateral growth with a predominantly reticulonodular pattern (a) and multifocal growth with ground-glass opacities (b).Fig. 16.46 Pulmonary lymphoma. Ill-defined large consolidations with air bronchograms.Fig. 16.47 Pulmonary metastases (renal cell carcinoma). Multiple pulmonary nodules with a lymphatic distribution pattern (i.e., distal to vessel endings due to a hematogenous spread).Fig. 16.48a, b Appearance pattern of lymphangitic carcinomatosis. Unilateral asymmetric nodular septal thickening (a), with centrilobular micronodules involving the subpleural space, patchy ground-glass opacities, and discrete pleural effusion on the right. Bilateral edema-like appearance with “crazy paving” (b).
Diagnostic pearls: Solitary (two thirds) or multiple (one third) round to oval nodules 1 to 5 mm in size. Nodules are well-defined, homogeneous, and typically slightly lobulated.
Nodules are surrounded by normal lung tissue. Often feeding arteries and draining veins are visible; thus, sequential contrast enhancement on dynamic CT is diagnostic.
Predilection for the medial third of the lung and for lower lobes.
Symptomatic only in the presence of multiple AVMs. Diagnosed usually in early adulthood either as an isolated anomaly or associated with Rendu–Osler–Weber syndrome (hereditary hemorrhagic telangiectasia).
The latter presents with telangiectatic changes in the skin and mucous membranes, epistaxis, and GI bleeding.
Vascular occlusion due to a thromboembolic disease often associated with an underlying cardiopulmonary disease.
Diagnostic pearls: Wedge-shaped, initially ill-defined, pleura-based consolidation with apex pointing toward the hilum (Hampton hump). “Melting ice block” sign: over time, consolidation becomes well defined and shrinks.
May occasionally cavitate.
After IV contrast administration often peripheral rim-like contrast enhancement of normal lung tissue.
Other findings supporting the diagnosis of pulmonary embolism include loss of lung volume with elevated ipsilateral diaphragm, ipsilateral oligemia (Westermark sign), ipsilateral pleural effusions, and enlarged central pulmonary arteries with evidence of intravascular clots on postcontrast scans.
Diagnostic pearls: Well-defined, round or lobulated mass in close proximity to the left atrium, as well as contrast enhancement simultaneous with the left atrium.
Histologically, a tortuous dilation of a pulmonary vein just before entering the left atrium.
May be acquired due to pulmonary venous hypertension or be congenital.
Inflammation
Amyloidosis
A variety of conditions in which amyloid proteins are abnormally deposited in the lung.
Diagnostic pearls:
Tracheobronchial type: Endobronchial nodules with obstructive airway disease.
Nodular type: Solitary or multiple nodules, partly with cavitation and/or calcification.
Diffuse parenchymal type: Diffuse interstitial disease of miliary or reticulonodular nature.
Histologically, deposition of fibrils of light-chain immunoglobulins in perivascular distribution. Primary amyloidosis (amyloid L) associated either with no disease or with multiple myeloma.
Secondary amyloidosis (amyloid A) associated with rheumatoid arthritis, TB, bronchiectasis, and Hodgkin disease.
Senile amyloidosis affects several organs, including lungs in elderly patients. Familial amyloidosis is rare.
Conglomerate masses ranging in the middle and upper lung zones and associated with a variety of pneumoconiosis.
Diagnostic pearls: Often bilateral but usually asymmetric.
Size ranges from 1 to 10 cm.
Lateral margin often sharply defined, medial margin usually ill-defined. Mass appears spindle-shaped, with a shorter anteroposterior and a longer mediolateral diameter.
Cavitation occurs due to either ischemic necrosis or superimposed TB.
Shrinkage of PMF affects compensatory surrounding emphysema with multiple centripetal pseudopodia originating from the mass.
Aggregation of smaller nodules indicates PMF.
It is found exclusively with pneumoconiosis, especially coal workers’ pneumoconiosis and silicosis, and less commonly with asbestosis.
However, in sarcoidosis, massive fibrosis may also present as a central homogeneous mass or large nodular lesions with irregular margins.
A form of necrotizing vasculitis affecting the lungs, kidneys, and other organs.
Diagnostic pearls: Multiple, usually sharply defined, bilateral nodules ranging from < 1 to 10 cm and commonly found in the lower lung zones; presence of “feeding” vessels entering the nodules; often thick-walled and nonregular cavitation that may progress into thin-walled cavities. Pleural effusions occur, but lymphadenopathy is rare. Endobronchial lesions cause segmental, lobular, and total lung atelectasis. Diffuse pulmonary hemorrhage may occur.
The limited form affects only the lungs.
The full mold also affects the kidneys and upper airways (nose and sinuses).
The lymphomatoid variant of Wegener granulomatosis typically spares the paranasal sinuses. Allergic granulomatosis (Churg–Strauss syndrome) presents as either multinodular disease or nonsegmental air-space consolidation in peripheral distribution, similar to eosinophilic pneumonia. Differential diagnosis: polyarteritis nodosa and necrotizing sarcoid granulomatosis, which may also present as multinodular disease.
Diagnostic pearls: Solitary or multiple, well- circumscribed, peripheral nodules measuring from 5 mm to 5 cm in diameter. Cavitation is common and may be thick or thin walled with a smooth inner lining.
Subcutaneous and pulmonary nodules may wax and wane simultaneously.
Caplan syndrome: Necrobiotic nodules and rheumatoid arthritis in patients with coal workers’ pneumoconiosis. These nodules may calcify.
Diagnostic pearls: Irregular mass or areas of consolidation containing regions of fat; often referred to as inflammatory pseudotumor.
May persist over months and mimic bronchogenic carcinomas.
May be exogenous (i.e., chronic aspiration of oil) or endogenous (cholesterol pneumonia). Similar inflammatory mass lesions but without fat entrapment are found with solid or liquid aspirations other than oil and in postobstructive pneumonitis.
Lung tissue separated from normal lung with blood supply from symmetric arteries and without participation in ventilation.
Diagnostic pearls: Well-defined heterogeneous mass in a posterior basal lower lobe segment, typically contiguous with the diaphragm; abnormal feeding vessels arise from the aorta, its side branches, or intercostal arteries.
Often single multicystic with or without air–fluid levels due to infection resulting from communication with the bronchial tree. Sequestered segments may show air trapping (left: 66%; right: 33%).
Intralobular sequestration usually presents in adulthood and is associated with other congenital anomalies (10%). Extralobular sequestration (20% of all sequestrations) characteristically presents as a homogeneous noncavitating mass in neonates often associated with other congenital anomalies. Venous drainage via systemic veins to the right heart. Differential diagnosis: venous drainage of intralobular sequestration via pulmonary veins.
A rare developmental anomaly of the lower respiratory tract.
Diagnostic pearls: Solitary or multiple, thin- or less commonly, thick-walled cystic mass; occasional presence of air–fluid levels; in the majority of cases, unilateral lung involvement with contralateral shift of the mediastinum. Absence of abnormal feeding and draining vessels may differentiate this condition from sequestration.
Intralobular mass of disorganized pulmonary tissue (mesenchymal and epithelial) with or without gross cyst formation. The pathogenesis of these tumors remains unknown.
Type I (50%): Single or multiple large cysts of variable size, often > 20 mm.
Type II (40%): Multiple small cysts of uniform size measuring < 12 mm.
Type III (10%): Solid mass without gross cyst formation (only microscopic cysts). Diagnosed in neonates and children. Associated in 25% with renal and GI abnormalities (especially types II and III). Multilobular involvement in 20%; middle lobe, however, is rarely affected.
Congenital atresia of a segmental bronchus with otherwise normal distal architecture.
Diagnostic pearls:
Classic triad: Mucus-filled bronchocele with hyperdistended and hypoperfused distal lung segment.
Mucus-filled bronchocele appears as a round/ovoid or lobulated well-defined perihilar mass.
Bronchocele nonenhancing on postcontrast scans.
Usually asymptomatic and discovered in screening chest radiographs in children and young adults.
CT clearly demonstrates the anomaly and may be used to confirm the diagnosis.
Characteristically affects apicoposterior segment of left upper lobe (< 50%), but also right upper lobe (20%), lower lobes (each 15%), and rarely right middle lobe (5%).
Diagnostic pearls: Single or multiple oval to spherical lesions ranging from 2 to 14 cm in diameter and presenting either as blood-isointense cystic lesions or thin-walled cavities with or without air–fluid level.
Typically observed in children and young adults after severe blunt chest trauma, but also after partial lung resection. Lesions usually develop immediately in the area of maximum impact, but may also occur hours to days after the trauma.
Focal lesion particularly in the apical/posterior segment of the upper lobes and associated with a TB infection.
Diagnostic pearls:
Tuberculoma: Smooth, well-defined, partly lobulated, round or oval nodule ranging in size from 1 to 4 cm. Small satellite lesions in the immediate vicinity of the lesion are common. Calcification occurs frequently.
Cavitary tuberculosis: Thin- to moderately thick-walled cavity with smooth inner lining. Fluid levels are rare. Surrounded by either air-space consolidation (i.e., local, exudative TB) or fibrotic changes with loss of volume and bronchiectasis (local fibroproductive TB). Pleural thickening (apical cap) is commonly associated.
Complication of cavitary TB includes bronchogenic spread of infectious material resulting in an exudative bronchopneumonia. Miliary TB due to hematogenous dissemination.
In 30% of adults with primary TB, cavitation is evident as air-space consolidation without site predilection, ipsilateral hilar adenopathy, and pleural effusion.
In atypical mycobacterial infections (e.g., MAI), cavities are more common and usually multiple.
Histoplasmosis
A fungal disease of the lung.
Diagnostic pearls: Histoplasmomas are one or several well-circumscribed nodules up to 3 cm in diameter with lower lobe predilection. Central calcification (“target lesion”) is characteristic.
Airborne spores of the fungus Histoplasma capsulatum are inhaled in the lungs, affecting local granulomatous reaction.
In case of cavitation, granulomas resemble tuberculomas and thus may be indistinguishable.
TB has an upper lobe predilection.
Echinococcosis (hydatid disease)
Solitary round to oval cystic mass measuring up to 10 cm in diameter.
Diagnostic pearls: Wall calcifications are not observed in lung lesions. “Crescent” sign due to air dissecting between cyst wall and surrounding lung tissue. “Water lily” sign: Cyst membrane may float on top of an air–fluid level or lie at the bottom after rupture of a cyst into a bronchus.
Infection with the larval form of Echinococcus multilocularis causing alveolar echinococcosis.
A complication of a GI infection with Entamoeba histolytica.
Diagnostic pearls: Right lower lobe consolidation often progressing into an abscess with a thick-walled cavity and irregular inner surface, as well as right pleural effusion.
An infectious disease caused by Entamoeba histolytica (a parasitic one-celled microorganism).
Pulmonary manifestation is a direct extension from a liver abscess through the diaphragm.
Aspergillosis covers a large spectrum of diseases, including pulmonary aspergilloma, allergic bronchopulmonary aspergillosis, and invasive aspergillosis.
Diagnostic pearls:
Aspergilloma: Round, solid, or spongelike mass within a preexisting cavity. Frequently found in the upper lobes. Scattered or fine rimlike calcifications occur. Allergic bronchopulmonary aspergillosis (ABPA): Mucous plugs within dilated (sub-) segmental bronchi producing a “cluster of grapes” or an inverted Y or V appearance. Often postobstructive airway disease.
Invasive aspergillosis: One, more often several ill-defined pulmonary nodules sitting at the distal end of a bronchus. Surrounding halo of low attenuation due to hemorrhage (invasion of vessels). Cavitation may affect an air crescent sign (air surrounding a sequestrum of necrotic lung) or a large empty cavity.
Aspergillomas are associated with chronic cavitary lung disease, particularly TB. May cause hemoptysis. ABPA is common in patients with asthma and cystic fibrosis. May result in widespread bronchiectasis and fibrosis. Invasive aspergillosis develops particularly in immunocompromised patients.
Bronchocentric granulomatosis may be considered a variant of ABPA and appears both clinically and radiologically in a similar fashion.
Diagnostic pearls: Solitary or multiple nodules between 0.5 and 5 cm in size (coccidioidomas). Predilection for middle and upper lung zones. May evolve into thin-walled cavities, typically located in the anterior segment of the upper lobes.
Primary coccidioidomycosis presents as consolidation preferentially in lower lobes with ipsilateral hilar adenopathy and small pleural effusion in 20% each. Disseminated coccidioidomycosis presents with a miliary pattern.
Diagnostic pearls: Large consolidation or mass measuring up to 10 cm in diameter with primarily lower lobe involvement. Development of large thick-walled cavities is a common feature.
Usually in debilitated or immunocompromised patients.
A common complication of actinomycosis and nocardiosis is empyema with subsequent rib and chest wall involvement.
Multiple well- or ill-defined, round or wedge-shaped subpleural lesions, more often with lower lobe predilection.
Diagnostic pearls: Involvement of the subpleural space and/or vessels entering the lesion is indicative of hematogenic spread. Thin-walled cavitation is frequent. Target sign: Air–fluid level and central hypoattenuation representing necrotic tissue highly suspicious of superinfection.
Most commonly caused by Staphylococcus or Streptococcus.
Often affects patients younger than 40. Predisposing factors include IV drug abuse, indwelling catheters, hemodialysis shunts, septic thrombophlebitis, endocarditis, osteomyelitis, and pharyngeal and pelvic infections.
Round pneumonia
Rare appearance of pneumonia.
Diagnostic pearls: Spherical air-space consolidation with air bronchograms and fluffy borders. Always in a posterior location, typically affecting the lower lobe.
Caused by Haemophilus, Streptococcus, or Pneumococcus.
Necrosis of pulmonary tissue and formation of cavities (> 2 cm) containing necrotic debris or fluid caused by microbial infection.
Diagnostic pearls: Locally decreased CT density surrounded by a consolidation is characteristic prior to cavitation.
Also characteristic are a hyperattenuating wall and a hypoattenuating (necrotic) center on postcontrast scans; and thick-walled cavitation with a shaggy inner lining in the acute stage, becoming smoother over time. Intracavitary air–fluid levels are common. Occasionally strands of residual lung tissue traversing the cavity may be present.
Often due to aspiration, which may occur during altered consciousness. Alcoholism is the most common condition predisposing to lung abscesses. Other causes include necrotizing pneumonias, bronchial obstruction with infection, and infected pulmonary infarcts. Lung abscess is considered primary (60%) when it results from an existing lung parenchymal process and is termed secondary when it complicates another process (e.g., vascular) or follows rupture of an extrapulmonary abscess into the lung.
Benign neoplasm composed of cartilage, connective tissue, muscle, fat, and bone.
Diagnostic pearls: Solitary, well-defined, often lobulated lesion in the lung periphery, measuring up to 10 cm in diameter. Endobronchial location in 10%. In 30%, stippled or conglomerate (“popcorn”) calcifications.
Focal intratumoral fat collections in 50%.
The most common benign neoplasm of the lung and the most common cause of solitary pulmonary nodule (5%–8%).
More common in men (preponderance 2:1 to 3:1). Peak incidence 60 to 70 y.
Usually asymptomatic and discovered incidentally. May rarely be associated with hemoptysis and cough. Multiple pulmonary fibroleiomyomata hamartomas is a related but extremely rare condition.
Papilloma (papillomatosis)
A benign lesion of the larynx and trachea.
Diagnostic pearls: Multiple or, less commonly, solitary endotracheal and endobronchial lesions with frequent cavitation. Obstructive pneumonitis and atelectasis are often associated with endobronchial location.
Usually arise in the larynx and spread distally In children and young adults, presenting with hoarseness and occasionally hemoptysis. Associated with human papilloma virus (HPV).
Recurrent respiratory papillomatosis is a rare, but acknowledged, risk factor for pulmonary squamous cell carcinoma.
A disease state defined by localized, irreversible dilation of part of the bronchial tree.
Diagnostic pearls:
Cystic/saccular: Thick-walled cystic spaces measuring up to 3 cm in diameter, usually with variable fluid levels. Cysts are either grouped together in a cluster or strung together in a linear fashion. Tubular/cylindrical: Thick-walled, dilated, nontapering crowded tubular structures (“tram lines”). “Gloved finger” appearance when filled with mucus. “Signet ring” appearance when viewed in cross section with a dilated, thick-walled bronchus producing the ring and the accompanying pulmonary artery branch the signet.
Varicose: Thick-walled, dilated bronchi with beaded contour.
Bronchiectasis is classified as an obstructive lung disease, along with emphysema, bronchitis, and cystic fibrosis.
Congenital: Kartagener or immotile cilia syndrome (situs inversus, sinusitis, and bronchiectasis), cystic fibrosis, chronic granulomatosis disease of childhood, alpha-1-antitrypsin deficiency.
Postinfectious: Chronic granulomatous disease (e.g., TB), measles, pertussis, Swyer–James syndrome (unilateral hyperlucent lung with decreased volume, air trapping, small ipsilateral hilum, and varicose bronchiectasis).
Postobstructive: Aspiration and fumes inhalation.
Cicatricial bronchiectasis is associated with advanced pulmonary fibrosis.
Reversible bronchiectasis refers to temporary dilation during pneumonia.
Bullae are cystic spaces > 1 cm in diameter confined by a hairline-thin wall that is visible in its entire circumference.
Diagnostic pearls: May be isolated or a component of advanced fibrotic lung disease or emphysema. Single large bulla occasionally isolated in the upper lobe.
May also be secondary to an evacuated pulmonary hematoma, old abscess, or bronchial cyst.
Pneumothorax is a frequent complication. Differential diagnosis: focal emphysema Blebs are cystic spaces, within the visceral pleura, usually above the apices, and not associated with lung destruction. They are rare and often the cause of a spontaneous pneumothorax.
Developmental foregut anomalies usually located within the mediastinum.
Diagnostic pearls: Solitary, well-defined, round or oval, homogeneous mass of water density (50%) or higher.
Measuring up to several centimeters in diameter. Most commonly located in the central (perihilar) portions of a lower lobe. Communication with the bronchial system occurs in 30% of cases, resulting in a thin-walled cystic lesion with or without an air–fluid level.
Although typically asymptomatic, infection or compression of adjacent structures may become prominent. Communication with the adjacent airways typically results in an infection, in which case the cyst fluid is replaced by pus and air. Infected congenital and acquired cysts (e.g., following lung abscess) cannot be differentiated except for a more widespread distribution of the latter.
Mesenchymal tumors
A group of endobronchial or small peripheral neoplasms with similar CT features but different histologic origin.
Diagnostic pearls: Well-defined small endobronchial or small peripheral nodules. Except for endobronchial lipomas (fat), findings are nonspecific.
Endobronchial lesions include granular cell myoblastomas, lipomas, leiomyomas, and lack of extrabronchial extension. Small peripheral nodules comprise fibromas, neurogenic tumors, and leiomyomas. Malignant variants of these tumors may very rarely also originate in the lung but usually represent hematogenous spread metastases from another region of the body.
A group of bronchial neoplasms that resemble each other grossly but are microscopically different.
Diagnostic pearls: Eighty percent arise within lobular, or (sub-) segmental bronchi, presenting as an endobronchial mass with frequent extension beyond the bronchial wall.
Postobstructive atelectasis and pneumonitis are the most common presentations. Postobstructive hyper-inflation is less common.
Peripheral adenomas (20%) are well-defined round lesions measuring 2 to 5 cm in diameter. Contrast enhancement may be considerable.
Diagnosed usually in patients between 30 and 50 y of age, often presenting with hemoptysis.
Comprise a variety of histologic subtypes, including carcinoids (90%), cylindromas (adenoid cystic carcinomas), mucoepidermoid carcinomas, and pleomorphic adenomas. These locally invasive, low-grade malignant tumors metastasize to regional lymph nodes and even distant sites. Kulchitsky cells are found in several of theses neoplasms, including carcinoids, atypical carcinoids, and small cell carcinomas in order of increasing malignancy.
A group of primary lung neoplasms with similar staging system but different histologic architecture.
Diagnostic pearls: Characterized by solitary peripheral or central mass, usually with irregular or spiculated border. Thick-walled cavitation with an irregular inner lining most commonly occurs with squamous cell carcinoma (15%). Eccentric calcifications are found in 5% and are caused by engulfment of a calcified granuloma or tumor necrosis.
Diffusely calcified mucinous adenocarcinomas are extremely rare.
Distal airway obstruction presenting as segmental, lobular, or lung atelectasis, and obstructive pneumonitis is found in 30% of the cases.
Air bronchograms are absent.
Endobronchial lesions or circumferential bronchial narrowing/occlusion are commonly demonstrated in central tumors. Pulmonary vessels may be occluded or contain tumor thrombi. Unilateral hilar adenopathy with or without mediastinal involvement is common and may be the only manifestation in 5% of cases, especially in small cell carcinomas.
Pleural effusions are present in 10% of cases at presentation. Localized or diffuse pleural thickening is occasionally found with peripheral tumors. Direct tumor extension into the chest wall, ribs, and vertebrae may also be evident in more advanced cases.
Classification:
1. Squamous cell (epidermoid) carcinoma (35%): Endobronchial lesion with airway obstruction (two thirds) or peripheral nodule (one third).
2. Adenocarcinoma (35%): Peripheral mass.
3. Small cell carcinoma (20%): Often small lung lesion with large hilar and mediastinal adenopathy.
4. Large cell carcinoma (15%): Large bulky peripheral mass.
TNM staging:
T0: No evidence of tumor
T1: Tumor < 3 cm
T2: Tumor > 3 cm or tumor with visceral pleural invasion or associated with obstructive pneumonia/atelectasis
T3: Tumor < 2 cm from carina, or invasion of parietal pleural, chest wall, diaphragm, mediastinal pleura, or pericardium
T4: Invasion of carina, heart, great vessels, trachea, esophagus, vertebral body, or malignant effusion
The least common of primary pulmonary carcinomas, and controversial as to its cell of origin.
Diagnostic pearls: The local form (75%) presents as a peripheral well-defined nodule when small (1–4 cm). Linear strands (pleural tags) may extend from a subpleural nodule to the pleura, representing a desmoplastic reaction with pleural indrawing. Larger lesions (> 4 cm) appear heterogeneous with air bronchograms and irregular margins (sunburst appearance). Often opacified vessels visible within the lesion on postcontrast scans. May be multifocal.
Ultrastructurally, all tumors are similarly composed of large cells with abundant cytoplasm and small nuclei in close contact with each other.
Pleural effusions and metastases to local lymph nodes and distant sites occur but are uncommon. Diffuse form (25%) presents as air-space consolidation often involving both lung fields.
Focal nodules primarily found in the presence of a hematogenous spread.
Diagnostic pearls: Pulmonary nodules range in size from miliary lesions to large well-defined masses (“cannonball” metastases).
Vessels entering the lesions are observed in ~30% of the cases.
Hilar or mediastinal lymphadenopathy is usually absent. Cavitation is rare, but it is characteristic of squamous cell carcinoma originating from the head, neck, or cervix.
Calcifications are also rare and occur typically in mucinous adenocarcinomas, osteosarcomas, synovial sarcomas, thyroid carcinomas (papillary and medullary), and malignant germ cell tumors.
A miliary pattern is usually associated with highly vascular metastases originating from carcinoma of the breast, thyroid, kidney, prostate, soft tissue, and chorion or bone sarcomas.
“Cannonball” metastases are typically associated with renal and colonic carcinomas, melanomas, and sarcomas. Ill-defined metastases due to hemorrhage are common in Kaposi sarcoma and choriocarcinoma. Endobronchial metastases presenting with airway obstruction occur with bronchogenic, renal, breast, and colon carcinomas and melanomas.
Solitary metastases are uncommon and typically originate from carcinomas of the colon (especially rectosigmoid area), kidney, testicles, and breast, sarcomas (especially bone), and melanoma.
Primary pulmonary disease is a rare disease, more often secondary pulmonary lymphoma.
Diagnostic pearls: The most common pulmonary manifestation is a coarse bilateral reticulonodular pattern resembling lymphangitis carcinomatosis (see also Fig. 16.46,p. 615).
Alternatively, multiple rather than solitary, poorly defined nodules or air-space consolidation with air bronchograms are found.
Pulmonary findings are usually associated with or subsequent to hilar and mediastinal lymph node involvement. Endobronchial lesions that may be associated with obstructive airway disease are rare. Pleural effusion occurs in 30% of cases and may be associated with circumscribed subpleural thickening.
Primary pulmonary lymphoma: Nodules with irregular margins or focal areas of consolidation, with air bronchograms.
Secondary pulmonary lymphoma: Thickening of interlobular septa, discrete pulmonary nodules, and areas of consolidation.
Hodgkin disease: Thin- or thick-walled cavities.
Primary pulmonary lymphoma is usually non-Hodgkin type; secondary pulmonary lymphoma is more common in patients with recurrent disease.
Recurrent or secondary pulmonary involvement may result from direct mediastinal nodal extension, from lymphatic or hematogenous dissemination from distant sites, or from foci of parenchymal lymphoid tissue.
Pseudolymphoma presents as localized interstitial or air-space disease with air bronchograms but without lymphadenopathy. It is a benign lymphomatous infiltration and can be considered as a localized form of LIP.
Plasmacytoma (primary of the lung) and secondary multiple myeloma manifestations are rare (1%) and similar to lymphoma.
Fig. 16.49 Arteriovenous malformation. A slightly lobulated subpleural mass is seen on the left side with a feeding vessel.Fig. 16.50a, b Pulmonary infarction. Wedge-shaped pleura-based consolidation dorsally in the right lower lobe (a) with corresponding pulmonary artery embolus (b).Fig. 16.51 Pulmonary varix. Note the enlarged pulmonary vein (arrow).Fig. 16.52 Progressive massive fibrosis (PMF) in sarcoidosis. A poorly marginated dense conglomerate mass is evident in the right midlung.Fig. 16.53 Wegener granulomatosis. Multiple thick-walled cavitary lesions with shaggy inner lining associated with small pleural effusions.Fig. 16.54 Rheumatoid necrobiotic nodule. A well-circumscribed, solitary peripheral nodule, which was removed and histologically proven. Cavitation is absent.Fig. 16.55 Pneumatocele. Solitary cystic lesion in the basal right lung due to obstructive overinflation associated with an acute pneumonia.Fig. 16.56 Lipoid pneumonia. Chronic bronchial obstruction of the left lower lobe with a pneumonia-like consolidation containing regions of fat (dark spots within consolidation).Fig. 16.57 Intralobular sequestration. A cluster of abnormal vessels in the posterobasal segment of the left lower lobe.Fig. 16.58 Intralobular sequestration. Irregular multiloculated cystic mass in the posterobasal segment of the left lower lobe.Fig. 16.59 Cystic adenomatoid malformation (type I). A large cystic mass in the anterobasal right upper lobe.Fig. 16.60a, b Congenital bronchial atresia. Hyperdistended and hypoperfused right middle lobe segment (a). Sagittal multiplanar reconstruction shows a mucus-filled bronchocele (b).Fig. 16.61 Lung cyst. Single thin-walled oval cavity without air–fluid level in the apical left lower lobe.Fig. 16.62 Cavitary tuberculosis. An ill-defined, thick-walled cavitary lesion in the posterior segment of the right upper lobe. The lesion is indistinguishable from a cavitating (squamous cell) bronchogenic carcinoma.Fig. 16.63 Amebiasis. A poorly marginated right lower lobe consolidation (arrow) surrounded by patchy parenchymal infiltrations and associated with a pleural effusion.Fig. 16.64 Aspergilloma. Round, solid mass within a preexisting cyst in the apical left lower lobe. Also visible is an invasive aspergillosis with central cavitation in the middle lobe.Fig. 16.65 Allergic bronchopulmonary aspergillosis (ABPA). Mucus plugs within dilated middle lobe bronchi producing an inverted Y or V appearance.Fig. 16.66 Invasive aspergillosis. Several ill-defined pulmonary consolidations at the distal end of right upper lobe bronchi. Note the surrounding halo of low attenuation due to hemorrhage (see also Fig. 16.63).Fig. 16.67 Coccidioidomycosis. Thick-walled solitary cavity located in the upper segment of the left lower lobe.Fig. 16.68 Nocardiosis. Large consolidation consisting of different-sized nodular lesions in the dorsal right lower lobe partly evolving into thick-walled cavities.Fig. 16.69a, b Septic emboli. Bilateral presence of ill-defined round to wedge-shaped subpleural lesions in the lower lobes (a). Ill-defined peripheral lesions and a small thin-walled cavitary lesion in the left lower lobe (b). Pleural effusions are present in both patients.Fig. 16.70 Lung abscess. A thin-walled, smooth cavity with an air–fluid level in the left lower lobe.Fig. 16.71 Hamartoma. A peripheral pulmonary nodule with a discrete calcification and focal intratumoral fat collections.Fig. 16.72 Cystic bronchiectasis. A cluster of thick-walled cysts in the left lower lobe with variable fluid levels.Fig. 16.73 Tubular bronchiectasis. The bronchiectasis appears as a thick-walled, dilated, nontapering tubular structure in the lingula resembling “tram lines.”Fig. 16.74 Bullae. Large cystic spaces are evident along the mediastinal pleura. They are confined by a hairline-thin wall, which is visible in its entire circumference.Fig. 16.75 Bronchogenic cyst. A solitary, well-defined, homogeneous round mass of water density is seen adjacent to the mediastinal pleura.Fig. 16.76 Bronchial adenoma, endobronchial type (carcinoid). The adenoma causes enlargement of the right upper lobe bronchus (arrow) and may be indistinguishable from other endobronchial lesions, such as papilloma and metastasis (see also Fig. 16.86).Fig. 16.77 Bronchial adenoma, peripheral type (carcinoid). The adenoma appears as a well-defined, peripheral round lesion.Fig. 16.78 Peripheral bronchogenic carcinoma (squamous cell carcinoma). Tumor < 3 cm in diameter. Also noted are beginning central cavitation, the presence of a pleural tail, and peritumoral carcinomatosis, all typical signs of malignancy (T1N0M0).Fig. 16.79 Peripheral bronchogenic carcinoma (adenocarcinoma). Tumor infiltration of the visceral pleural and extensive ipsilateral mediastinal lymphadenopathy. Pleura effusion separates visceral from parietal pleura (T2N2M0).Fig. 16.80 Peripheral bronchogenic carcinoma (squamous cell carcinoma). A large irregular cavitating mass in the apical right lower lobe, < 2 cm from the carina, with distinct peritumoral carcinomatosis and invasion of the parietal pleural (T3N0M0).Fig. 16.81 Central bronchogenic carcinoma (small cell carcinoma). Large endobronchial mass is evident within the right main bronchus, already bulging into the trachea. Associated with this are complete atelectasis of the right lung, infiltration and occlusion of the pulmonary artery, extensive mediastinal lymphadenopathy, and concomitant pleural effusion (T4N3M0).Fig. 16.82 Pancoast tumor. A large inhomogeneous mass in the apex of the left lung with destruction of the adjacent vertebral body and posterior rib.Fig. 16.83 Local alveolar cell carcinoma. An ill-defined, patchy peripheral consolidation is seen in the right lower lobe.Fig. 16.84 Multiple lobulated metastases. Multiple lobulated metastases seen in a patient with breast carcinoma.Fig. 16.85 Cannonball metastases. Cannonball metastases seen in a patient with soft tissue sarcoma.Fig. 16.86 Endobronchial metastasis (melanoma). A nodular lesion in the right lower lobe bronchus (arrow). Densities in the right lower lobe are caused by obstructive pneumonia (melanoma).Fig. 16.87 Solitary metastasis (colon carcinoma). Well-defined round lesion in the right middle lobe.Fig. 16.88 Calcified pulmonary metastasis. A nodule with irregular calcifications is seen in the right lower lobe (chondrosarcoma).Fig. 16.89 Primary pulmonary lymphoma. Several poorly defined nodular densities with air bronchograms.
Only gold members can continue reading. Log In or Register to continue