16 Malformations and Deformities
Anomalies of the skeleton and soft tissues of the hand can be caused by congenital malformations or deformities acquired during growth. The most important malformations are associated with syndactyly, brachydactyly, oligodactyly, polydactyly, aphalangia, constriction rings, hypoplasia/aplasia of the thumb, macrodactyly, symphalangism, camptodactyly, clinodactyly, phocomelia, clubhand, and cleft hand. If other organs are involved additionally, the anomalies arereferred to as malformation syndromes. Deformities that appear later in life include several entities of localized dysostosis, the best known of which is Madelung deformity, systemic manifestations of osteochondrodysplasia, which are characterized by disproportional short stature, sclerosing and hyperostotic bone lesions, and different forms of dysostosis multiplex, which are primarily due to metabolic disorders.
Pathoanatomy and Clinical Symptoms
According to the most appropriate classification and nomenclature of morphological defects, a malformation is a primary structural defect resulting from a localized error in embryonic (rarer in fetal) morphogenesis. The symptoms of malformation are already manifest at birth. Malformation syndrome denotes the sum of all of a person’s malformations that have the same etiology but different pathomorphogeneses. In contrast, a deformity summarizes all secondary changes in shape and structure that have developed from an originally normally developed body part.
Congenital malformations of the upper extremities are rare and are seen in only about 1 of 600 newborns. Ten percent of these are functionally severe deformities. Inherited factors (endogenous causes) must be differentiated from environmental factors (exogenous causes). Examples of hereditary malformations of the hand are the Apert syndrome and trisomy 21. An example of an exogenous factor is the drug thalidomide, which causes longitudinal arrest of the upper extremities ranging from aplasia of the thumb to aplasia of the entire extremity (amelia). In approximately 40–50% of all malformations, the causes remain unknown.
Diagnostic Imaging
Imaging usually consists of radiographs of both hands and forearms. However, in newborns and small children, radiographic diagnosis is limited because the ossification nuclei of the hand first appear between the second month and fourth year of life. In the future, high-resolution ultrasonography and MRI may provide hand surgeons with important information about the nonossified skeletal sections and soft tissues for early surgical intervention. A simple photograph of the malformed hand, preferably in functional position, provides valuable documentation.
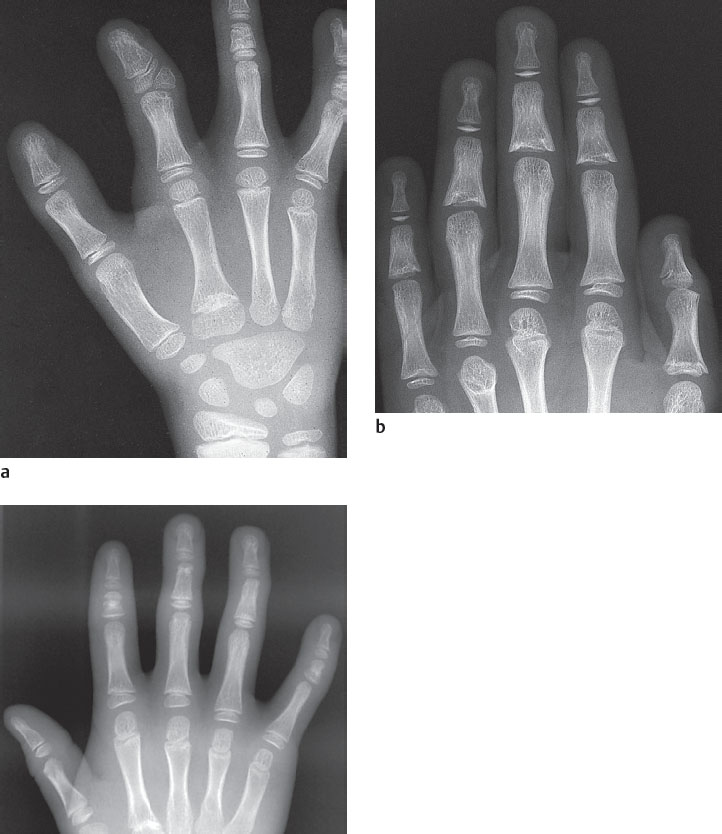
We stress here also the changes in form and structure at the epiphyses and metaphyses, which appear either as isolated asymptomatic variants or in combination with further imaging signs, and may be diagnostically relevant for the recognition of a malformation (Fig. 16.1c):
Pseudoepiphyses serve as an example of epiphyseal lesions. These are constitutionally incompletely formed epiphyses that on radiographs show no continuous growth plates. Another epiphyseal lesion consists of epiphyses or epiphyseal notches in abnormal sites (Fig. 16.1a). Except in the thumb, epiphyses are normally located on the distal ends of the metacarpals and on the proximal ends of the phalanges. Epiphyses at abnormal sites occurring together with a hypoplastic thumb and brachymesophalangia/clinodactyly V can serve as indications of a hand-foot-uterus syndrome.
Congenital changes of the metaphyses (Fig. 16.1b) must be differentiated from acquired forms. Irregular metaphyses adjacent to the growth plates are often seen in healthy children, especially on the middle and distal phalanges. These metaphyseal changes, together with osteosclerosis, are seen in delayed epiphyseal closure. Increased metaphyseal osteosclerosis, which is probably caused by testosterone, is far more common in boys than girls.
Chapters 49 and 50 summarize the different changes in form and structure of the epiphyses and metaphyses.
Classification
Congenital malformations of the hand can be classified either according to their etiology or according to morphological criteria. The following classification systematically considers the seven categories of both the International Federation of Societies for Surgery of the Hand and the International Society for Prosthetics and Orthotics. These categories of malformation are listed in Table 16.1 together with their incidences.
Malformation | Incidence (%) |
Failure of formation | 12.2 |
Failure of differentiation | 31.3 |
Duplication | 35.9 |
Overgrowth | 0.5 |
Undergrowth | 4.3 |
Constriction ring syndrome | 6.5 |
Generalized abnormalities (syndromes) | Variable |
Disease Entities
Failure of Formation
Transverse Arrest
All forms of congenital amputation are considered transverse arrests (the upper arm and proximal forearm are not considered here). In the following forms of transverse arrest, parts of the carpus, the metacarpus, or the fingers are missing.
Aphalangia indicates one or more missing fingers. It occurs either sporadically as a solitary malformation or in combination as in numerous malformation syndromes, in cleft hand, in symbrachydactyly, and in the constriction-ring syndrome (see Figs. 16.8 and 16.19 ). An important differentiating criterion of the constriction-ring syndrome is the absence of distal finger parts, including the fingernails, in contrast to the other forms of aphalangia in which the distal finger parts are rudimentarily developed.
A related malformation is oligodactyly. In oligodactyly, not only a finger is missing(aphalangia) but also an entire metacarpal of the affected ray (Figs. 16.1a and 16.2 ). Oligodactylies are usually combined with further malformations, i.e., brachydactyly (shortening of the finger ray), syndactyly (fusion of adjacent finger rays), symbrachydactyly (a group of malformations with shortening, thickening, and partial or complete absence of phalanges, in some cases combined with fusion of adjacent finger rays), carpal synostosis, and other malformations of the forearm including tendon and muscle anomalies.
Longitudinal Arrest
All other forms of an incomplete arm and hand skeleton, including the intercalated segments, are defined as defects of longitudinal development.
Phocomelia: In this longitudinal defect, the upper arm and/or the forearm (as an intercalated segment) is completely missing. The hand skeleton is attached to a shortened and functionally restricted upper extremity. In phocomelia, the degree of severity ranges from total type (arrest of both the upper and lower arm), proximal type (arrest of the upper arm only), and distal type (arrest of the forearm only).
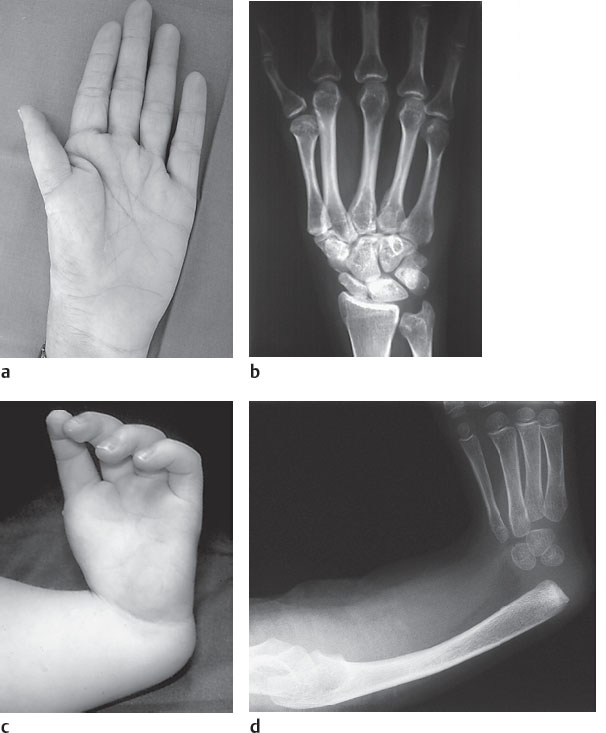
Radial (preaxial) ray deficiency (“radial clubhand”): In radial ray deficiency, the radius may be hypoplastic, partially absent, or completely absent, with or without a deficient thumb (Fig. 16.2c, d). Because of the missing radial forearm support, the wrist deviates to the radial side with the extent of deviation depending on the degree of radial ray deficiency. A genetic defect is not known; in 50–70% of cases, the radial clubhand is bilateral. In unilateral radial clubhand, the contralateral thumb can be hypoplastic. The elbow is often fixed in extension. The proximal interphalangeal joints of the radial fingers are restricted in their mobility because the strength of the digital flexor muscles is diminished at the level of the deformed wrist. Furthermore, the extrinsic carpal and digital muscles—the flexors as well as the extensors—and additionally the muscles of the upper arm and shoulder girdle can be either atrophic or fused. The variance of radial ray deficiency is broad, ranging from mild hypoplasia to complete absence of the radius, of the thumb, or of the radial carpals, combined with a deformed humerus, a bent and shortened ulna, and an elbow fixed in extension. Accordingly, one or several of the radiographic signs listed in Table 16.2 can be present.
Additional anomalies are often combined with radial ray deficiency, particularly heart defects (e.g., the Holt-Oram syndrome) and diseases of the hematopoietic system (e.g., thrombocytopenia and Fanconi anemia). Appropriate screening should therefore be conducted in the presence of radial clubhand. Accompanying congenital anomalies are triphalangia, hypoplasia or aplasia of the thumb, and, less commonly, of the fingers, as well as carpal or radioulnar synostoses.
Ulnar (postaxial) ray deficiency (“ulnar clubhand”): Ulnar ray deficiency is a sporadic congenital malformation of the ulnar segments of the forearm and hand. This anomaly is relatively rare. Owing to the absent or insufficient humeroulnar articulation, the articulation of the elbow is usually severely disturbed, while the carpus remains stable. Different degrees of severity may occur. Typical radiographic signs, which can be seen separatelyor in combination, are listed in Table 16.3 .
A shortened cartilaginous anlage of the ulna is considered the cause for ulnar deviation of the hand. In addition to instability or synostosis of the elbow, other musculoskeletal malformations are often present.
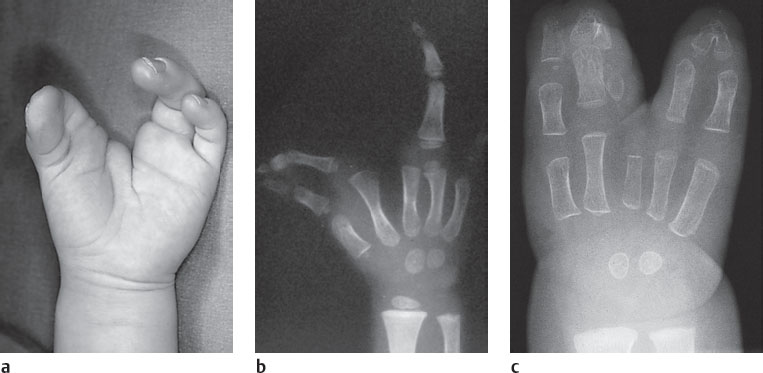
Central ray deficiency (“cleft hand”): Formally, this anomaly is a peripheral cleft of the hand skeleton ranging from an intermetacarpal division between the middle and ring fingers to aplasia of the middle finger (Fig. 16.3a). Hypoplasia of the radial fingers (median or medioradial type) to syndactyly of the remaining fingers can additionally be present. Cleft hand is often accompanied by an adducted thumb, metacarpal transverse bones that encumber the cleft by forming triangles, and syndactyly between metacarpals I and II, as well as between metacarpals IV and V. Characteristically, manifestations are bilateral on the hands and feet, and a family history of this malformation can be demonstrated. Cleft feet and cheilognathopalatoschisis (cleft lip, gums, and jaw) often accompany central ray deficiency.
In differential diagnosis, symbrachydactyly must be excluded, particularly symbrachydactyly of the so-called cleft-hand type (Fig. 16.3c), which is different from clubhand both in genetics and in manifestation ( Table 16.4 ).
|
Failure of Differentiation (Separation) of Parts
Symphalangy
In general, symphalangy describes restriction in movement of a finger. This anomaly is usually congenital and is often located in the proximal interphalangeal joint as ankylosis (see Fig. 16.9 ). Autosomal-dominant inherited symphalangy predominantly affects one or more fingers on the ulnar side. There is often also a short middle phalanx, whose growth plate must not be confused with the joint space. Nonhereditary symphalangy is associated with syndactyly, Apert syndrome, or Poland syndrome.
Camptodactyly
Camptodactyly is defined as a congenital, usually bilateral, flexion deformity of a finger that occurs either sporadically or through autosomal-dominant inheritance. Camptodactyly is most often located in the proximal interphalangeal joint and in the little finger (Fig. 16.5a). Several fingers are usually affected in the presence of arthrogryposis. Pathoanatomically, there are abnormal insertions of the lumbrical muscles or the superficial digital flexor tendons. The malalignment of the affected finger slowly becomes apparent clinically in early childhood or youth. The metacarpophalangeal joint is often hyperextended in compensation. The radiographic signs listed in Table 16.5 often affect the joint secondarily several years later. The lateral radiograph must be taken in a strictly lateral position and centered on the affected joint.
In flexion the thickened base of the middle phalanx fills the palmar notch on the neck of the adjacent proximal phalanx, causing compensatory hyperextension of the metacarpophalangeal joint.
Clinodactyly
In clinodactyly, the finger ray is bent to the radial or ulnar side in such away that the tip of the affected finger points to the middle of the hand (see Figs. 16.8a, 16.14 , 16.19 , 16.20 ). The anatomic cause is a deformed middle phalanx with nonparallel articular surfaces. The little finger, the index finger, and the triphalangeal thumb are most often affected. Clinodactyly can be an isolated phenomenon or can be combined with numerous malformation syndromes. Depending on the extent of the lateral deviation and the shortening of the finger, three degrees of severity can be differentiated.
Two special forms should be mentioned:
In the delta phalanx, which represents grade III of clinodactyly, the phalanx has a delta or triangular shape. The growth plate runs in longitudinal direction from proximal to distal ( Fig. 16.4 ). The diaphysis is on the convex side of the clinodactylic finger and is surrounded by the C-shaped growth plate over a long distance on the concave side (longitudinally bracketed diaphysis).
In Kirner deformity, which must be differentiated from clinodactyly, the distal phalanx of the little finger deviates to the radial and palmar aspects (Fig. 16.5c,d). This sporadic deformity primarily affects females and is manifested bilaterally. Radiographs reveal a delayed closure of the growth plate and increased osteosclerosis.
|


Pollex Flexus
Pollex flexus denotes a congenitally bent thumb. In this case, radiographs are not very informative. Pollex flexus has two variations:
One is the trigger thumb, caused by an interphalangeal joint fixed in flexion. The pathoanatomy of this immobile malposition is the presence of small nodules on the flexor pollicis longus tendon proximal to the anular ligament A1. Surgical splitting of the anular ligament is normally required. In rare cases, trigger pathology can be found on the other finger rays.
The other anomaly is the clasp thumb (pollex flexus congenitus), which also affects the metacarpophalangeal joint. The minor variant of the hook-shaped thumb is caused by hypoplasia or aplasia of the extensor muscles of the thumb. The more complex variant iscaused by a number of pathologic factors: hypoplasia of the extensor tendons, flexion contracture of the metacarpophalangeal joint, laxity of the ulnar collateral ligament, hypoplasia or aplasia of the thenar muscles, adduction contracture at the carpometacarpal joint, and cutaneous lesions in the first interdigital space. The complex clasp thumb is often associated with ulnar deviation and flexion of the other metacarpophalangeal joints, as well as with radiocarpal hyperextension. This results in the “windblown” deformity ( Fig. 16.6 ) and in the Freeman-Sheldon syndrome in which a facial deformity is also found.
Arthrogryposis Multiplex Congenita
Congenital contractures of the upper and lower extremities with flexed and immobile joints are characteristic of arthrogryposis. Passive movement is alsorestricted. This anomaly is caused by pathology of the second neurons between the spinal anterior-horn cells and the motor endplates. The severity of arthrogryposis depends on the degree of disease expression, as listed in Table 16.6 .


Syndactyly
In syndactyly, two or more neighboring fingers are fused by their soft tissues and/or osseous structures. This entity is the most common malformation of the hand. In addition to sporadic forms, there are dominantly inherited forms of syndactyly with different degrees of expression. Half of the cases have bilateral manifestations. The incidence of syndactyly between fingers I and II is 5%, between fingers II and III is 15%, between fingers III and IV is 50%, and between fingers IV and V is 30%. Depending on the extent of fusion and other accompanying malformations, the following variants of syndactyly mustbe differentiated:
In complete syndactyly, the adjacent fingers are fused over a long distance, including the distal phalanges (with or without fusion of the fingernails). Complete syndactyly is the most common fusion anomaly (Fig. 16.8a).
In incomplete syndactyly, the fingers are fused over a shorter distance distal to the middle of the proximal phalanges and not including the distal phalanges.
In simple syndactyly, there is no synostosis but only fusion of the phalangeal soft-tissues (webbed fingers).
Complex syndactylies are characterized by osseous fusions. Complex syndactylies can be combined with further malformations of the fingers such as oligodactyly and polydactyly, symphalangism (Fig. 16.8b), brachydactyly, and cleft hand. The following subtypes can be differentiated:
Acrosyndactyly is a distal cutaneous or osseous fusion located between two distal phalanges. The proximal phalanges remain separated (Fig. 16.8c). Accompanying brachydactyly can also be observed.
Oligosyndactyly and polysyndactyly are seen in a number of malformation syndromes. These are phalangeal fusionson the hands with a reduced or increased number of fingers. Polysyndactylies are usually associated with accessory rays of the middle and ring fingers (see page 169 Central Polydactyly), and they are rarely seen in preaxial and postaxial forms.
Symbrachydactyly includes combined malformations with phalangeal fusion (syndactyly) and short fingers (brachydactyly)( Figs. 16.9 and 16.11 ). Symbrachydactyly is most often seen on two or three ulnar fingers and is characteristically not inherited. A further characteristic is the unilateral manifestation on the hand and foot. The often stumpy fingers have fingernails. Several subtypes of symbrachydactyly are differentiated according to the degree of manifestation ( Table 16.7 ).
A cleft hand must be differentiated from symbrachydactyly because, apart from being inherited, there are differences in the distribution and localization. Extreme manifestations of both variants are monodactyly I (Fig. 16.9b), which is classified as a subtype of symbrachydactyly, and monodactylyV, which is a special subtype of the cleft hand ( Table 16.4 ).
Apert syndrome (acrocephalodactyly type I), which is dominantly inherited, is a combination of bilateral syndactyly with symphalangism and brachydactyly ( Fig. 16.9 ) as well as with acrocephaly and hypertelorism. The thumb is often included in the syndactyly, or it may carry a delta phalanx with radial inclination. In syndactyly of fingers II–V, the affected fingers can share a single fingernail. The maximal manifestation of Apert syndrome includes all phalanges and the thumb, and is called “spoon hand.” It is frequently seen.
The nonhereditary Poland syndrome ( Fig. 16.11 ) denotes a unilateral hypoplastic hand with syndactyly (the middle phalanges are usually missing) combined with aplasia of the pectoral muscle and hypoplasia of the shoulder girdle.
Other syndactyly syndromes are acrocephalodactyly types II-V, Carpenter syndrome (acrocephalopolysyndactyly), and the oculodentodigital syndrome (Chapter 51).

|


The probability of more peripherally located and abnormal divisions of the digital vessels and nerves increases with the degree of severity of a syndactyly (see Fig. 48.16 ).

As a rule, carpal fusions (synostoses) are of only minor functional relevance. As described in Chapter 15, these are merely variants of the normal carpus. Synostoses of the proximal sections of the metacarpals are very rare.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


