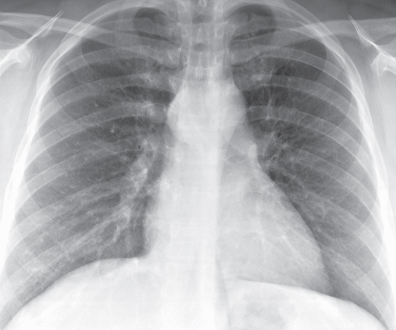
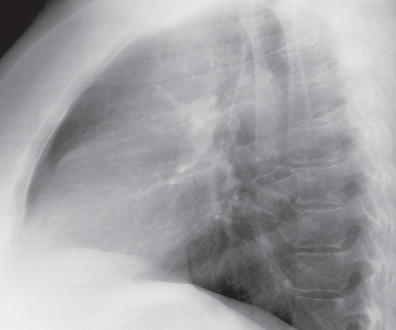
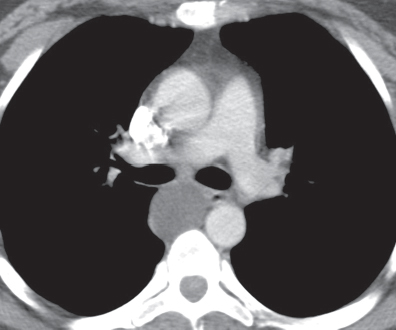
CASE 162 25-year-old woman with cough PA (Fig. 162.1) and lateral (Fig. 162.2) chest radiographs demonstrate a well-defined middle-posterior mediastinal (subcarinal) mass that projects to the right of the midline on the frontal chest radiograph and projects over the posterior subcarinal region on the lateral chest radiograph. Contrast-enhanced chest CT (mediastinal window) (Fig. 162.3) shows a spherical fluid attenuation cystic lesion in the posterior subcarinal region with minimal discontinuous enhancement of a thin cyst wall. Bronchogenic Cyst • Other Foregut-Derived Cysts; Esophageal, Gastroenteric • Pericardial Cyst • Lymphadenopathy Congenital cysts represent approximately 20% of mediastinal masses affecting adults. Bronchogenic cyst is the most common congenital mediastinal cyst and is typically located in the middle-posterior compartment near the carina, but may also affect other mediastinal compartments, the pericardium, diaphragm, pleura, or lung. Other foregut-derived congenital cysts include esophageal duplication cysts, which occur in the wall of the esophagus and middle-posterior mediastinum, respectively. Pericardial cysts are typically located in the cardiophrenic angle. Thymic cysts usually affect the anterior mediastinum and often represent acquired lesions. Fig. 162.1 Fig. 162.2 Fig. 162.3 Congenital cysts are typically unilocular thin-walled lesions with a variable fluid content. Bronchogenic cyst is thought to result from abnormal budding of the primitive foregut or the developing tracheobronchial tree. The original connection to the foregut is usually obliterated resulting in a blind-ending fluid-filled thin-walled cyst. Esophageal duplication cysts may also derive from the primitive foregut as a result of anomalous esophageal development. Pericardial cysts are thought to result from disordered formation of the primitive coelomic cavities. While unilocular thymic cysts probably represent congenital anomalies related to the fetal thymopharyngeal duct, multilocular thymic cysts are generally considered acquired lesions related to trauma (including thoracotomy), thymic neoplasia, and radiation therapy for lymphoma. Multilocular thymic cysts affect approximately 1% of children infected with HIV in association with diffuse infiltrative lymphocytosis syndrome. They are also described in other immune-mediated disorders (e.g., Sjögren syndrome, aplastic anemia, myasthenia gravis). Patients with bronchogenic cyst are typically young children and adults under the age of 40 years. Many are symptomatic and present because of chest pain and/or respiratory complaints related to mass effect on the airways. Patients with esophageal cysts are often asymptomatic adults and children, but some present with symptoms of esophageal/mediastinal mass effect or with local pain related to ectopic gastric mucosa in the cyst wall. Patients with pericardial cysts are invariably asymptomatic and diagnosed incidentally. Patients with thymic cysts are often asymptomatic children and young adults.
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine



