17 Arachnoid Cysts
17.1 Case Presentation
17.1.1 History and Physical Examination
A 35-year-old woman presents with a history of recent-onset headaches.
Neurological examination was normal.
17.2 Imaging Analysis
17.2.1 Imaging Findings and Impression
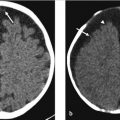
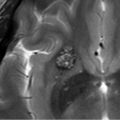
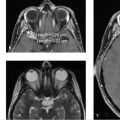
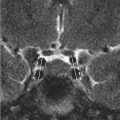
MRI with and without contrast shows an oblong extra-axial lesion in the left anterotemporal fossa (asterisks). The lesion follows cerebrospinal fluid (CSF) signal intensity (hyperintense on T2, hypointense on T1 with suppression of the content on fluid-attenuated inversion recovery [FLAIR]) on all spin-echo sequences (▶ Fig. 17.1a–c). On postcontrast images (▶ Fig. 17.1d,e), the lesion does not demonstrate any enhancement. Findings are consistent with middle cranial fossa arachnoid cyst.

17.2.2 Imaging Guidelines
MRI with and without contrast is the diagnostic examination of choice. Contrast should be administered for initial diagnostic evaluation in the cases in which diagnosis is unclear (atypical findings, edema of the underlying brain, patient symptoms are concerning for infection) to exclude nodular peripheral enhancement.
CT is better for evaluating adjacent bony changes like thinning of overlying skull but not necessary.
Not recommended: CT with contrast (unless MRI with contrast contraindicated).
17.3 Clinical Evaluation and Management
This is a young, healthy woman with a small, incidentally found Galassi type I arachnoid cyst. No surgical intervention is needed at this time because the cyst is small without any mass effect and the patient’s symptoms cannot be clearly attributed to the cyst. Small arachnoid cysts (< 5 cm) such as this are low risk for rupture or hemorrhage. 1 We would plan to reimage the cyst in 3 months to check for any change in cyst size or morphology. If stable, we would obtain one more MRI in 1 year and then follow the patient clinically and only obtain additional imaging if new symptoms arose.
17.4 Differential Diagnosis
Arachnoid cyst:
Well-circumscribed, extra-axial mass that follows CSF signal intensity on MRI and is isodense to CSF on CT with no enhancement identified. 2
Epidermoid cyst:
It is a congenital lesion occurring due to inclusion of ectodermal elements during neural tube closure.
On imaging, it appears as a lobulated extra-axial lesion with a tendency to insinuate between structures rather than cause mass effect in earlier stages.
On CT, it may be indistinguishable from an arachnoid cyst as epidermoid cysts exhibit CSF density similar to an arachnoid cyst. Some epidermoid cysts (10–25%) demonstrate internal calcification.
On MRI, epidermoid cysts follow CSF signal intensity on T1-weghted image (T1WI) and T2-weghted image (T2WI); however, there is incomplete suppression of the signal on FLAIR, giving a “dirty” CSF appearance. 3
On diffusion-weighted imaging (DWI), it demonstrates bright signal with corresponding dark signal on apparent diffusion coefficient (ADC), due to presence of thick waxy epithelial keratin within the cyst.
It may show minimal enhancement around the periphery of the lesion.
Porencephalic cyst:
It occurs after traumatic/ischemic insult to the brain parenchyma.
It follows CSF signal intensity on all sequences. However, it is surrounded by gliotic brain.
Choroid fissure cyst:
It has a typical location and is believed to arise from the choroid epithelium.
It can be indistinguishable from an arachnoid cyst.
Racemose neurocysticercosis:
It is rare in the western world.
There is absence of scolex in racemose neurocysticercosis as opposed to intraparenchymal lesions.
They are larger than intraparenchymal lesions since these occur within CSF spaces and their growth is not restricted by relatively noncompliant brain.
They may conglomerate to appear as a bunch of grapes.
Cysts associated with neoplasms:
Various tumors like pleomorphic xanthoastrocytoma, ganglioglioma, and dysembryoplastic neuroepithelial tumor (DNET) can present as mixed solid and cystic mass lesions and can mimic an arachnoid cyst when the solid component is negligible.
However, these tumors are usually cortical in origin and demonstrate signs of being an intra-axial mass lesion (absence of CSF cleft, absence of buckling of underlying cortex, presence of edema in the surrounding area, etc.).
Moreover, these lesions will demonstrate enhancement of the solid component after gadolinium administration.
17.5 Diagnostic Pearls
CT: Extremely well circumscribed, with an ill-defined wall, and displace adjacent structures. When large, and over time, they can exert a remodeling effect on the bone.
MRI: Follow CSF signal intensity on all sequences and no enhancement can be identified. 2
Magnetic resonance cisternography: high-resolution T2 W sequences help delineate the cyst wall and adjacent anatomic structures. 4
Lack of restriction of diffusion on DWI is most important to help distinguish arachnoid cysts of the cerebellar pontine angle from epidermoids.
17.6 Essential information about arachnoid cysts
17.6.1 Etiology
It is known to arise from within the leaves of arachnoid membrane.
Arachnoid cysts can occur anywhere within the central nervous system, most frequently (50–60%) located in the middle cranial fossa, where they may invaginate into and widen the sylvian fissure.
Other locations include the suprasellar cistern, ventricles, posterior fossa, cisterna magna, cerebellopontine angle, and spinal canal.
They are most frequently solitary.
Posttrauma, arachnoid cyst can grow in size from increased intracystic fluid accumulation secondary to ball valve mechanism or secretory activity of arachnoid cells.
17.6.2 Galassi Classification
Galassi et al, 5 in 1982, described three types of middle cranial fossa arachnoid cysts based on the size, shape, mass effect on the surrounding brain parenchyma and communication with subarachnoid space on cisternography. It still remains the most widely used classification system in practice.
The three types of arachnoid cysts are as follows:
Type I: These are spindle shaped and smaller in size as compared to the other two types. They are located in anterior most part of temporal fossa and impose minimal to mild mass effect and displacement of the adjacent temporal lobe. On cisternography, they show free communication with the subarachnoid space (▶ Fig. 17.2).
Type II: These are triangular or quadrangular in shape. They occupy the anterior and middle part of the temporal fossa with marked mass effect on the temporal lobe. Slow communication with subarachnoid space can be demonstrated on cisternography (▶ Fig. 17.3).
Type III: These are the most severe form of arachnoid cyst. They are round or oval in shape. They occupy almost the entire temporal fossa with extensive displacement of the temporal lobe and even frontal and parietal lobes to some extent. Little communication with subarachnoid space is seen on cisternography (▶ Fig. 17.4).



Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


