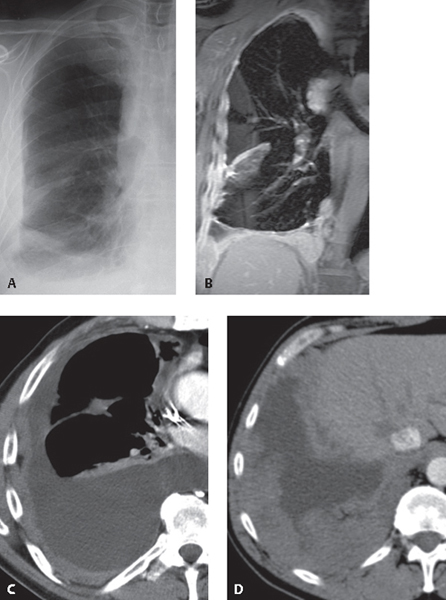
CASE 175 83-year-old man with malaise and right-sided pleuritic chest pain Coned-down PA chest radiograph (Fig. 175.1A) demonstrates a moderate right pleural effusion and moderate pleural thickening along the lateral right pleural surface that extends into the interlobar fissure. Coronal T2-weighted MR image (Fig. 175.1B) shows circumferential right pleural thickening by high-signal nodular masses. Note extension into the interlobar fissure and right costodiaphragmatic recess, involvement of the mediastinal pleura, and invasion of the diaphragm and mediastinum. Contrast-enhanced chest CT (mediastinal window) (Figs. 175.1C, 175.1D) reveals the right pleural effusion; extensive plaque-like and nodular pleural thickening along the costal, diaphragmatic, and mediastinal pleural surfaces; and nodular involvement of the minor fissure. Fig. 175.1 Diffuse Malignant Pleural Mesothelioma • Pleural Effusion of Non-Neoplastic Etiology • Malignant Pleural Effusion; Pleural Metastases (adenocarcinoma, carcinoma of other cell type, lymphoma) Diffuse malignant pleural mesothelioma is a relatively rare pleural malignancy. It is the most common primary pleural neoplasm. The majority of cases of malignant pleural mesothelioma (80–90%) are related to the carcinogenic effects of asbestos, and most lesions occur in individuals with documented occupational or environmental asbestos exposure. Approximately 6% of asbestos workers will develop mesothelioma. While a higher incidence of mesothelioma is observed in patients with continuous exposure to asbestos, intermittent, brief, and indirect exposures have also been implicated in the development of this neoplasm. Occupations with increased exposure to asbestos include construction, shipyard, and insulation work. The latency period between onset of exposure and development of mesothelioma is between 20 and 40 years. Both amphibole and chrysotile asbestos fibers are associated with the development of mesothelioma. Amphiboles are long, needle-like fibers that penetrate deeply into the lung, resist clearance, and are considered more tumorogenic than the serpiginous chrysotile asbestos fibers.
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


