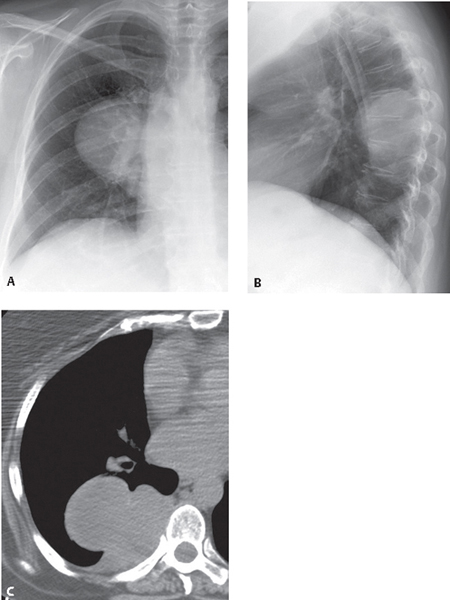
CASE 177 Asymptomatic 67-year-old man Coned-down PA (Fig. 177.1A) and lateral (Fig. 177.1B) chest radiographs demonstrate a mass in the posterior right hemithorax. The mass has well-defined lateral and superior borders (Figs. 177.1A, 177.1B) and an indistinct inferior border (Fig. 177.1B). The lesion’s inferior obtuse angles with the adjacent pleura result in incomplete border visualization on the lateral radiograph (incomplete border sign). Unenhanced chest CT (mediastinal window) (Fig. 177.1C) shows a well-defined homogeneous, lobulated soft-tissue mass that forms obtuse angles with the adjacent pleura. There is no evidence of chest wall involvement. Fig. 177.1 Localized Fibrous Tumor of the Pleura • Other Mesenchymal Pleural Neoplasm • Chest Wall Neoplasm (schwannoma, neurofibroma) • Pleural Metastasis Localized fibrous tumors of the pleura are rare but represent the second most common primary pleural neoplasm after mesothelioma. They probably arise from submesothelial mesenchymal cells that undergo fibroblastic differentiation. While most are related to the pleura, they have also been described in other intra- and extrathoracic locations. Localized fibrous tumors are not related to mesothelioma or to asbestos exposure. Localized fibrous tumors are neoplasms of unknown etiology. Localized fibrous tumors typically occur in adult men and women in the fifth through eighth decades of life. Many patients (particularly those with small tumors) are asymptomatic and diagnosed incidentally because of an abnormal chest radiograph. Symptoms typically relate to tumor size and include cough, chest pain, and dyspnea. Constitutional symptoms, hypoglycemia, clubbing, and hypertrophic osteoarthropathy rarely occur. • Well-defined lobular nodules/masses; typically abut the pleura (Figs. 177.1A, 177.1B)
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
Imaging Features
Chest Radiography
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


