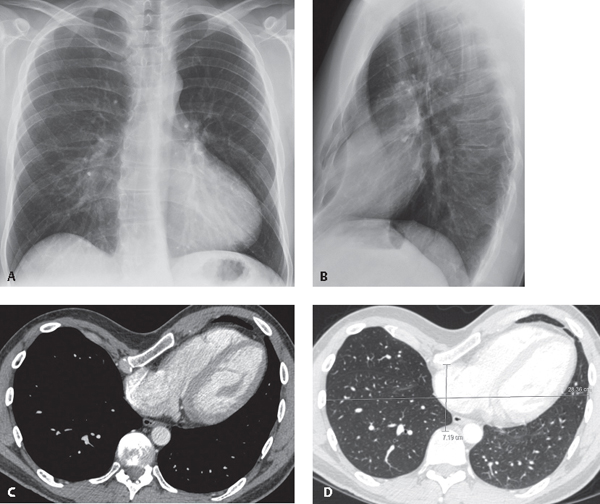
CASE 183 Asymptomatic 35-year-old man PA (Fig. 183.1A) and lateral (Fig. 183.1B) chest radiographs demonstrate a severe pectus excavatum deformity. Note vertical orientation of the anterior ribs and obscuration of the right cardiac border in the absence of right middle lobe consolidation. Contrast-enhanced chest CT (mediastinal window, Fig. 183.1C; lung window, Fig. 183.1D) reveals the pectus deformity, with posterior displacement of the sternum and associated leftward displacement of the heart (Fig. 183.1C). The illustrated anteroposterior (7.19 cm) and transverse measurements (28.36 cm) (Fig. 183.1D) are used to compute the Haller (pectus) index (see below). Pectus Excavatum Fig. 183.1 None Pectus deformities (pectus excavatum and pectus carinatum) are among the most common chest wall anomalies in the general population. There is great variability in the anatomy and morphology of the anterior chest wall of asymptomatic children. Thus, mild asymmetry and mild degrees of pectus deformity are sometimes considered normal variants. Pectus excavatum is also referred to as “funnel chest.” Pectus excavatum is thought to result from abnormal growth of the costal cartilages that produces depression of the sternum (typically its inferior portion) often associated with sternal rotation to the right. Typically, there is associated rotation and displacement of the heart and mediastinum to the left. Pectus carinatum and localized pectus excavatum probably result from sternal growth disturbances with or without associated costal cartilage abnormalities. Severity of pectus excavatum may be determined by computing the Haller index (syn. pectus index), which is defined as the ratio of the transverse diameter (horizontal distance of the inner aspect of the rib cage) and the anteroposterior diameter (shortest distance between the anterior cortex of the vertebrae and the posterior cortex of the sternum at its narrowest point). In the illustrated case (Fig. 183.1D), the pectus index is 4 (28/7). A pectus index over 3.25 is one of the parameters used to select candidates for surgical correction of the chest wall deformity. The normal Haller index is about 2.5.
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


