24 Carpometacarpal Dislocations and Fracture-Dislocations
Carpometacarpal (CMC) dislocations and fracture-dislocations affect one or several joints, the little finger and dorsal dislocations being most involved. Extensive ligament tears occur. Because of the bidirectional overlapping of CMC structures in the radiographic projectional views, the complete extent of trauma is often first seen in computed tomography (CT).
Pathoanatomy and Clinical Symptoms
The CMC joints of fingers II–V are rarely injured. Strong force is required to cause dislocation or fracture-dislocation of these joints because of the strong carpometacarpal and intermetacarpal ligaments. Carpometacarpal shearing forces occur when a horizontal force is applied to the metacarpus while the carpus is fixed to a solid resistance or vice versa. In impact and compression traumas, the force is transferred along the metacarpal axis, typically resulting in fracture-dislocations.
The pattern of injury includes either isolated fingers or, in about 80% of cases, several fingers. The little finger is most often affected (50%), followed by the index finger (ca. 25%). The more common dorsal CMC dislocations are differentiated from the rarer palmar ones according to the direction of the force applied.
Main clinical signs are acute pain and functional disability, as well as bony deformity of the hand, in which either a step deformity can be felt on the dorsum of the hand or the palm is flattened. Damage to the ulnar and median nerves is observed in palmar CMC dislocations. Chronic subluxations lead to a loss of finger strength and pain independent of loading.
Diagnostic Imaging
Radiography
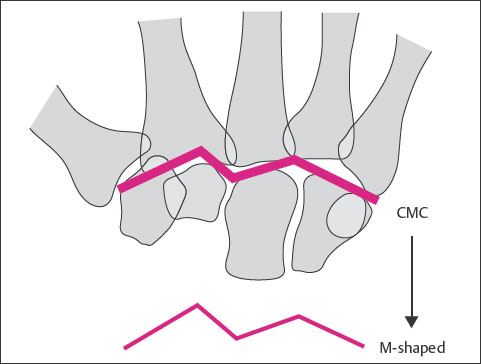
A discrepancy is often between the generally impressive clinical findings and obviously unremarkable findings on radiographs. This is caused by the overlapping of the CMC joints in radiographic survey views. The CMC transition region must, therefore, be systematically analyzed according to the following radio-anatomic characteristics ( Table 24.1 and Fig. 24.1 ).
These radiographic signs are reliable only when the palm is laid flat on the film cassette with straight fingers. It is often difficult to analyze the x-rays of patients following trauma because, as a result of pain and swelling, the dorsopalmar view cannot be exposed with the palm pressed flat on the cassette. In this situation, the dorsopalmar semipronated oblique view and the palmodorsal semisupinated oblique view are often helpful.
Transverse to the longitudinal axis:
|
Parallel to the longitudinal axis:
|
Pattern of Trauma | Direction of Dislocation |
CMC dislocation |
|
CMC fracture-dislocation |
|
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


