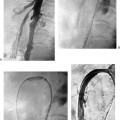
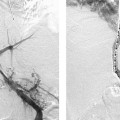
CASE 25 A 76-year-old male presented to the emergency room with flank pain and a fever of 101°F. He was referred to the radiology department for noninfused CT angiography (CTA) to exclude nephrolithiasis. Figure 25-1 Aortic infection with pseudoaneurysm formation. (A) Noninfused CT shows inflammation on the posterior wall (arrows) of the aorta. (B) Infused CT obtained 10 days later shows a saccular aneurysm with increased inflammation. (C) Frontal aortogram shows saccular aneurysm. (D) Lateral aortogram shows pseudoaneurysm to better advantage. A noninfused CT study was performed and revealed a small amount of inflammation adjacent to the posterior abdominal aorta at the level of the mid-kidneys (Fig. 25-1A). The significance of this finding was uncertain, and the patient was sent home to receive close follow-up. Symptoms persisted, and a repeat infused CT exam was obtained 10 days later. This scan demonstrated marked progression of the inflammatory process and a new saccular aneurysm (Fig. 25-1B). The patient was then referred to the vascular and interventional radiology section for abdominal aortography. The right common femoral artery was catheterized using the Seldinger technique and a 5-French (F) pigtail catheter was advanced into the midabdominal aorta. Aortography was performed in frontal and lateral projections using 30 cc of contrast injected at 20 cc/s. Aortography revealed a juxtarenal saccular aneurysm (Figs. 25-1C, D). Aortic infection with juxtarenal saccular aneurysm formation. The patient was taken to the operating room. The midabdominal aorta was resected and oversewn, and grafts were fashioned to the major visceral arteries. An axillobifemoral bypass graft was performed to provide arterial flow to the legs. The patient was placed on long-term antibiotics. Cultures of the resected specimen grew Salmonella. Infected aneurysms or pseudoaneurysms of the aorta are rare. The classic triad of fever, pain, and pulsatile mass is found in fewer than half of affected patients. The term “mycotic aneurysm” is a misnomer as most infections are due to bacteria, not fungus. Salmonella is the most common causative agent of aortic infections; unlike most bacteria, Salmonella can invade the arterial intima. Staphylococcal aureus
Clinical Presentation
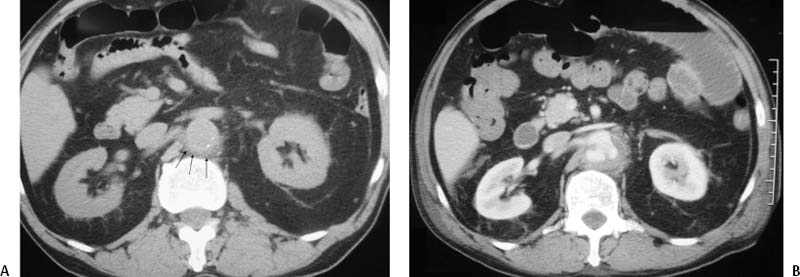

Radiologic Studies
Angiography
Diagnosis
Treatment
Discussion
Background
![]()
Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


