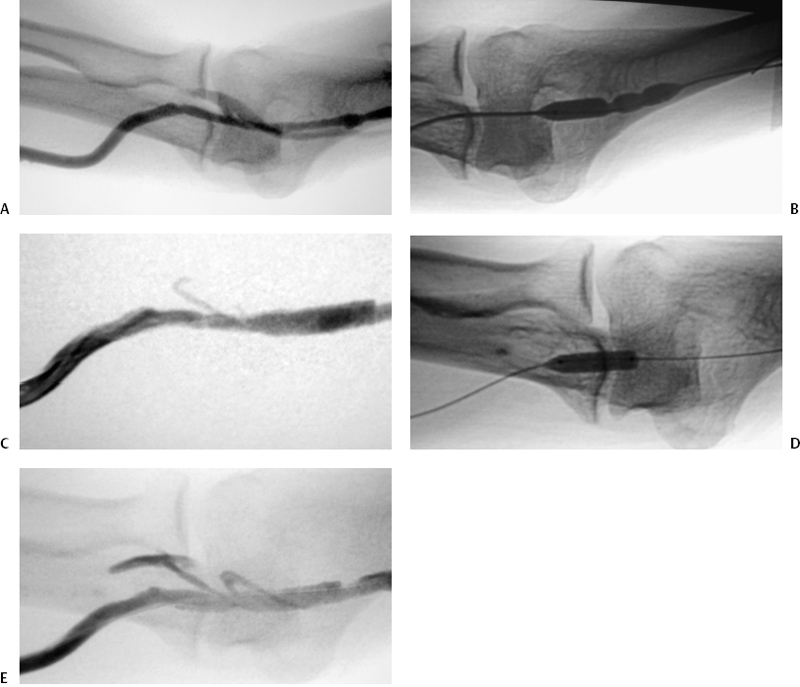
CASE 3 A 43-year-old male with a forearm dialysis graft was referred to interventional radiology for evaluation of high venous pressures at dialysis. Physical examination of the arm revealed a patent graft with a bounding pulse. Figure 3-1 Cutting balloon angioplasty of hard-to-dilate venous stenoses. (A) Initial digital subtraction venogram shows venous stenoses in the peripheral outflow at the level of the elbow. (B) Fluoroscopic image shows high-pressure angioplasty balloon failing to fully dilate stenoses. (C) Follow-up digital subtraction venogram after initial angioplasty shows residual narrowing at site of angioplasty. (D) Fluoroscopic image shows cutting balloon angioplasty of refractory stenoses. (E) Follow-up digital subtraction venogram after cutting balloon angioplasty shows wide patency of venous outflow. The forearm graft was punctured using a Micropuncture set (Cook, Bloomington, Indiana) and the needle was exchanged over a 0.018-inch guidewire for a 5-French (F) dilator that was used to perform fistulography. The fistulagram revealed multiple stenoses of the proximal venous outflow at the level of the elbow (Fig. 3-1A). Venous outflow stenoses. A 7-mm × 4-cm high-pressure angioplasty balloon (Blue Max, Boston Scientific, Natick, Massachusetts) was advanced to the stenoses and inflated to 24 atmospheres. The lesions could not be fully expanded (Fig. 3-1B). Follow-up venography demonstrated persistent narrowing of the outflow vein (Fig. 3-1C). A 7F sheath was placed via the existing access site in the graft and a 0.018-inch guidewire was advanced across the residual stenoses. A 7-mm × 2-cm cutting balloon was advanced to the lesions and inflated to 8 atmospheres (Fig. 3-1D). Follow-up venogram showed wide patency of the segment without residual stenoses (Fig. 3-1E). Cutting balloon: 5 to 8 mm in diameter and 1 or 2 cm in length. Maximal recommended inflation pressure is 10 atmospheres. 7F sheath 0.018” guidewire Contrast material
Clinical Presentation
Radiologic Studies
Diagnosis
Treatment
Equipment
Discussion
Background
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


