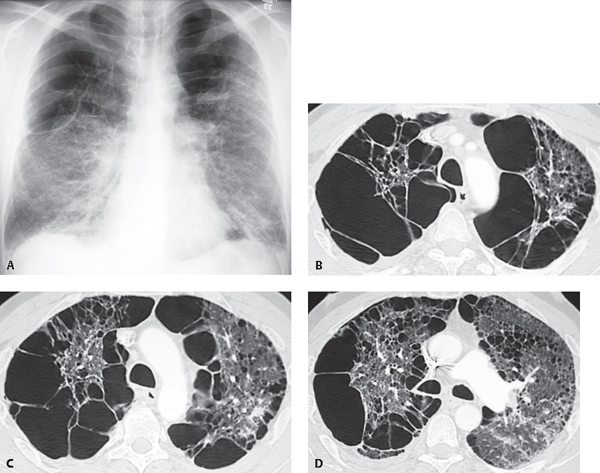
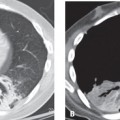
CASE 30 46-year-old man with dyspnea PA chest radiograph (Fig. 30.1A) demonstrates hyperinflation with bilateral upper lobe hyperlucency secondary to bilateral large apical bullae that compress adjacent lung. Bands of atelectasis are demonstrated at both lung bases. High-resolution CT (lung window) (Figs. 30.1B, 30.1C, 30.1D) demonstrates bilateral large bullae that preferentially affect the right lung and produce mediastinal shift to the left. Scattered areas of proximal acinar emphysema and a single subpleural arcade of distal acinar emphysema are demonstrated in the left upper lobe (Fig. 30.1D). Fig. 30.1 Bullous Lung Disease and Distal Acinar Emphysema None Distal acinar (paraseptal) emphysema is the least common type of emphysema and, together with proximal acinar emphysema, is frequently associated with the formation of bullae. It affects the periphery of the acinus (Fig. 30.2) adjacent to the subpleural upper lobe interlobular septa and is usually an incidental imaging finding. Adjacent foci of paraseptal emphysema may coalesce to form bullae. A bulla is defined as a sharply demarcated air-containing space measuring 1.0 cm in diameter or more in the distended state. Bullae are characteristically thin-walled (1 mm) and may be unilocular or compartmentalized by thin septa. Bullae may be solitary or multiple and most commonly occur in the lung apex. Multiple adjacent subpleural bullae may mimic distal acinar emphysema. The term giant bullous emphysema refers to bullae that occupy at least one-third of a hemithorax. The pathogenesis of distal acinar emphysema is uncertain but is probably related to a relative paucity of vascular and elastic fibers in subpleural pulmonary lobules.
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


