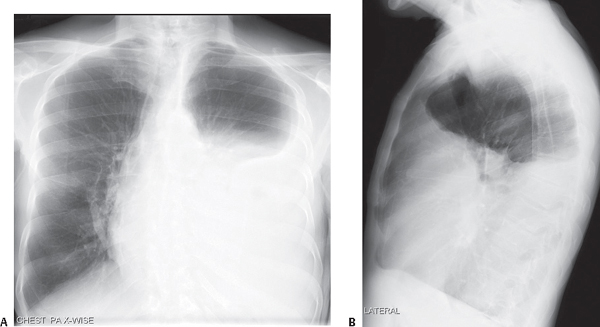
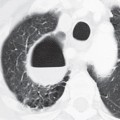
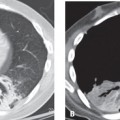
CASE 34 72-year-old man with long-standing history of chronic obstructive lung disease presents to his physician with progressive dyspnea over the last several weeks and left-sided pleuritic chest pain PA (Fig. 34.1A) and lateral (Fig. 34.1B) chest X-rays show opacification of nearly two-thirds of the left hemithorax. Note the airless left mid- and lower thorax and contralateral mediastinal shift from this pleural space-occupying process. The lateral exam (Fig. 34.1B) also demonstrates a positive spine sign characterized by increased opacity over the lower thoracic spine and obscuration of the left diaphragm. Relaxation Atelectasis Lingula and Left Lower Lobe; Left Pleural Effusion (Empyema) • Atelectasis • Parenchymal Consolidation Fig. 34.1 Relaxation (passive) atelectasis occurs when there is loss of contact between the visceral and parietal pleurae by a space-occupying process (e.g., pleural effusion, pneumothorax) exerting extrinsic pressure on the parenchyma. The elastic recoil properties of the lung preserve its shape as it loses volume. In the absence of pleural adhesions, the degree of atelectasis is proportional to the volume of fluid (Fig. 34.2C) or air (Fig. 34.3) in the pleural space. Mantle
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
![]()
Stay updated, free articles. Join our Telegram channel



Full access? Get Clinical Tree


