35 Renal Mass
35.1 Case 1
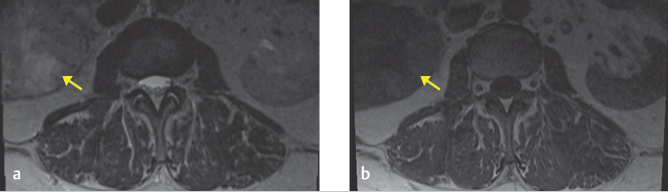
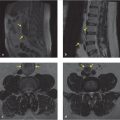
A 63-year-old woman presents with lower back and bilateral lower extremity pain. An MRI of the lumbar spine without contrast was performed to evaluate for radiculopathy.
35.1.1 Imaging Impression
An ill-defined right renal mass is incompletely evaluated in this noncontrast lumbar spine MR examination (▶ Fig. 35.1). The appearance is worrisome for malignancy and additional imaging is required.
35.1.2 Diagnostic Testing Needed
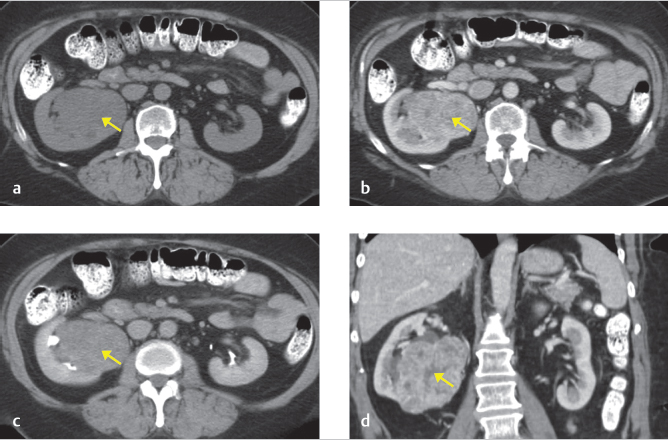
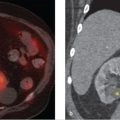
Given that an incompletely characterized right renal mass without diagnostic features of a simple cyst is visualized, additional imaging is required and a CT renal mass protocol was subsequently performed with findings compatible with a 6-cm right renal cell carcinoma (RCC) shown in ▶ Fig. 35.2.
35.1.3 Imaging Interpretation
A right expansile 6-cm arterially enhancing renal mass with washout compatible with an RCC.
35.2 Case 2
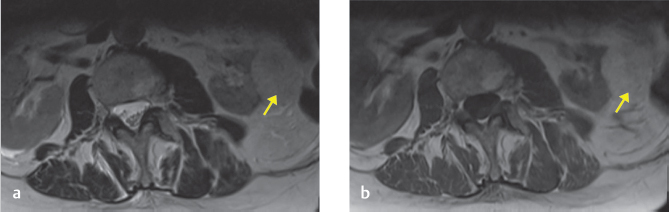
An 80-year-old woman presents with back pain after a fall. MRI of the lumbar spine without contrast was performed for evaluation.
35.2.1 Imaging Impression
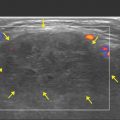
A left renal mass with high T1 and T2 signal is incompletely evaluated by the noncontrast lumbar spine MRI (▶ Fig. 35.3). As the signal intensity of this mass does not follow that of fluid, and it is incompletely imaged, additional imaging is required.
35.2.2 Additional Testing Needed
The finding of a left renal mass without imaging characteristics of a renal cyst on MRI (well-marginated and homogeneously high in signal on T2 and low in signal on T1 weighted images) requires additional imaging to exclude malignancy. If the lesion was detected on a lumbar spine CT without intravenous contrast, incomplete imaging, heterogeneity, or internal density measurements between 20 and 70 HU, it would require additional imaging. The ACR recommends CT scan with and without intravenous contrast or MRI pre- and postcontrast, especially if the lesion is < 1.5 cm. 1 , 2 , 3 Given that the lesion is T1 and T2 hyperintense, there is suggestion of a fat-containing lesion like an angiomyolipoma. If there had been a fat-saturated sequence (frequency selective), the presence of signal loss in the left renal lesion would be compatible with an angiomyolipoma with macroscopic fat. Angiomyolipomas can also contain microscopic fat, and loss of signal in the opposed-phase image in chemical shift MR will confirm that finding.
Unlike microscopic fat-containing RCCs, angiomyolipomas typically do not contain calcifications. Therefore, a fat-containing mass in the kidney without calcifications most likely represent an angiomyolipoma.
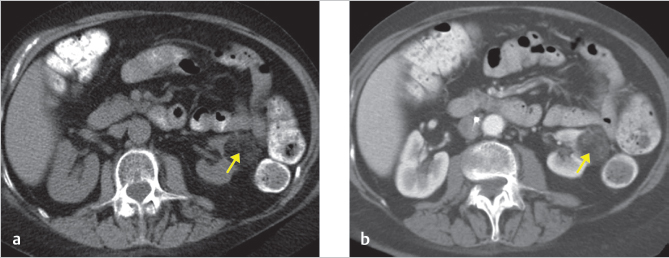
Fortunately, a CT with and without contrast was performed about 10 years prior to the MRI and that CT demonstrated a left renal fat-containing lesion with macroscopic fat without calcifications, compatible with a macroscopic fat-containing angiomyolipoma. On the other hand, a lesion with macroscopic fat and calcification within the kidney is highly suspicious for a RCC. No further imaging was necessary, given that the lesion was less than 4 cm. However, if that lesion were larger than 4 cm, there is a propensity for bleeding and the blood supply to these lesions are typically embolized, especially if a renal artery aneurysm is greater than 0.5 cm. 3 , 4
35.2.3 Imaging Interpretation
Left renal lesion containing macroscopic fat, compatible with a 3.8-cm renal angiomyolipoma.
35.3 Differential Diagnosis
Differential diagnosis (DDx) for lesions of the kidney are presented in ▶ Table 35.1.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


