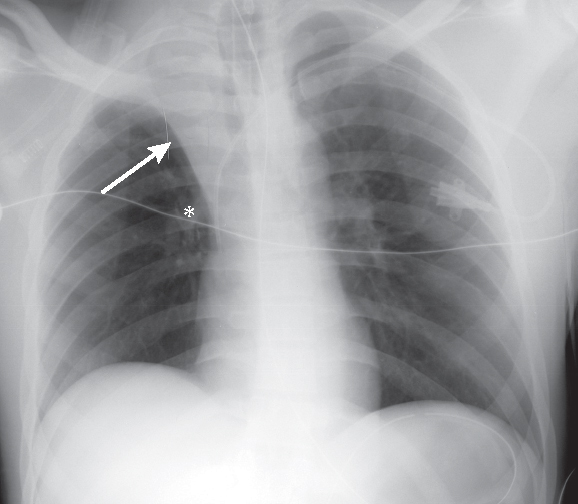
CASE 37 38-year-old man status post recent abdominal surgery requiring ventilator support with an abrupt drop in oxygen saturations and decreased breath sounds over the upper right thorax AP chest radiograph (Fig. 37.1) shows cephalad displacement of the horizontal fissure (arrow) and elevation of the right hilum (asterisk) and diaphragm. Note the decrease in volume of the right hemithorax and the ipsilateral mediastinal shift. Right Upper Lobe Atelectasis; Obstructing Mucus Plug • Aspirated Foreign Body (e.g., tooth) Fig. 37.1 The horizontal fissure and upper half of the oblique fissure approximate by shifting upward and forward, respectively (Fig. 37.2). On lateral chest radiography, both fissures appear gently curved. The horizontal fissure assumes a concave configuration inferiorly, whereas the oblique fissure may appear convex, concave, or flat (Fig. 37.2). On frontal radiography, the horizontal fissure maintains a superiorly convex morphology. With increased volume loss, the horizontal fissure continues to move up, over the apex of the thorax, and the collapsed lobe becomes contiguous with the superior mediastinum. In total lobar atelectasis, the volume of the collapsed right upper lobe may be so small that the atelectatic lobe mimics superior mediastinal widening on the frontal chest exam (Figs. 37.2, 37.3
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
![]()
Stay updated, free articles. Join our Telegram channel



Full access? Get Clinical Tree


