CASE 37 A newborn presents with mild respiratory grunting. Figure 37A Figure 37B Frontal (Fig. 37A1) and lateral (Fig. 37A2) chest radiographs in a newborn with mild tachypnea reveal a uniform, well-marginated opaque mass in the posterior aspect of the base of the left hemithorax. CT examination shows a low attenuating left basal mass and an enhancing systemic artery supplying it, which arises from the descending thoracic aorta (Fig. 37B). This proved to be an extralobar pulmonary sequestration. Extralobar pulmonary sequestration Pulmonary sequestration is a mass of aberrant pulmonary parenchymal tissue that has no normal connection to either the tracheobronchial tree or the pulmonary arterial system. Sequestrations receive their blood supply from the systemic arterial system and have variable pulmonary or systemic venous drainage. There are two types that are defined according to their pleural investiture: extralobar sequestration (~25%) is contained within its own pleural lining, whereas intralobar sequestration (~75%) shares the pleura with the rest of the lung. It is therefore thought that an extralobar sequestration appears after pleura is formed, whereas the intralobar variety may form earlier, that is, before pleura is formed. Presentation may occur through a variety of mechanisms. Traditionally, most extralobar sequestrations present earlier in life with respiratory difficulty, whereas the majority of sequestrations present in older age ranges with superinfection of the lesion. Many of these lesions, however, are now detected by prenatal ultrasound examination. Some clinical differences between intralobar and extralobar sequestrations include a male predominance when the sequestration is extralobar (80%), whereas intralobar sequestrations occur equally in males and females. As well, extralobar sequestrations in the neonatal period have an approximate 65% incidence of other congenital anomalies, which occur in only 10% of children with intralobar sequestrations.
Clinical Presentation
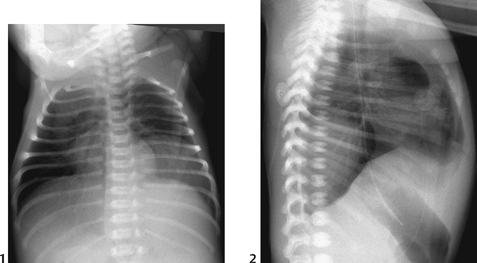
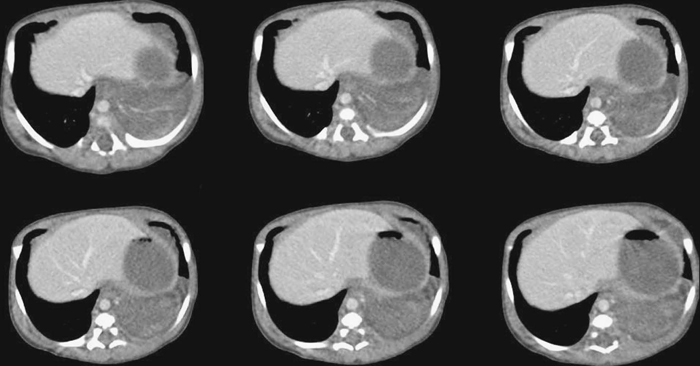
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Imaging Findings
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


