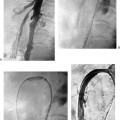
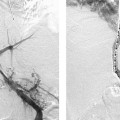
CASE 37 A 69-year-old diabetic female had rest pain involving the right leg. She had a long history of peripheral arterial occlusive disease but had not had previous surgery. Her ankle-brachial index was 0.3. Physical exam revealed limb atrophy, decreased skin temperature, and rubor. She slept with the right foot over the side of the bed on the floor. She was referred for CT angiography (CTA) runoff. Figure 37-1 CTA of superficial femoral artery stenoses. (A) Axial image shows concentric lesion (circle) of right superficial femoral artery. (B) Surface-shaded reconstruction shows tandem superficial femoral artery lesions (arrows). Note that the more distal lesion is difficult to appreciate due to the adjacent femur. (C) Maximal intensity projection reconstruction shows tandem superficial femoral artery lesions. Using a 64-slice helical scanner, CT arteriography was performed. The exam revealed two high-grade stenoses of the distal right superficial femoral artery (Fig. 37-1). The infrapopliteal vessels were also diseased although there was continuous runoff to the right foot via a peroneal artery. Endovascular intervention was planned. Tandem stenoses of the right superficial femoral artery. The left common femoral artery was catheterized using the Seldinger technique, and a 6-French (F) sheath was inserted. The right common femoral artery was then selectively catheterized over the bifurcation using a 5F RC-1 catheter (Boston Scientific, Natick, Massachusetts) and arteriography of the right leg was performed. Views of the superficial femoral artery demonstrated the two stenoses detected on CTA (Fig. 37-2A). Five thousand units of heparin were administered intra-arterially. Nitroglycerine in 200-μg aliquots were given intra-arterially throughout the procedure to minimize vasospasm. The 6F sheath was advanced over the bifurcation into the contralateral common iliac artery to provide additional mechanical advantage. The lesions were crossed with a 0.035-inch Bentson guidewire (Cook, Bloomington, Indiana) and 5F MPA catheter (Cook, Bloomington, Indiana). Injection via the sheath (not shown) after crossing both lesions revealed that the catheter was occlusive to flow. The Bentson wire was then replaced by an exchange length (260 cm) 0.035-inch Rosen guidewire (Boston Scientific, Natick, Massachusetts) and a 5- × 20-mm angioplasty balloon catheter was advanced to the site of the stenoses. Both lesions were dilated sequentially beginning with the more proximal stenosis (Fig. 37-2B). The angioplasty catheter was then removed leaving the guidewire across the lesion. An angiogram performed via the 6F sheath revealed resolution of the stenoses (Fig. 37-2C). Puncture needle
Clinical Presentation
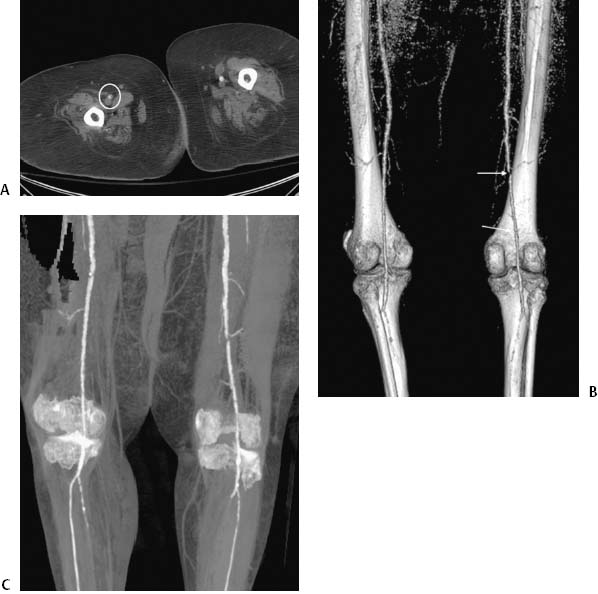
Radiologic Studies
CTA Runoff

Diagnosis
Treatment
Angioplasty
Equipment
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


