Kaustubh G. Shiralkar, Eduardo J. Matta, Steven S. Chua, and Chakradhar R. Thupili
39.1 Case 1
39.1.1 History
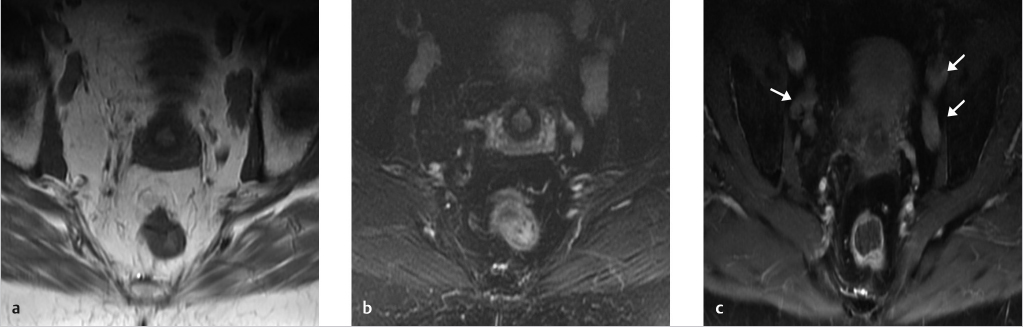
A 67-year-old woman presents with chronic back pain. MRI of the sacrum with and without intravenous (IV) contrast was performed to evaluate for possible nerve root compression (▶ Fig. 39.1).
Fig. 39.1 T1-weighted nonfat saturation (a), T2-weighted fat saturation (b), and postcontrast T1-weighted fat saturation (c) axial images demonstrate bilateral enlarged lymph nodes within the iliac chain (arrows). These nodes are enlarged measuring up to 2 cm in short-axis diameter. There is homogeneous enhancement without evidence of necrosis.
39.1.2 Most Likely Imaging Diagnosis for Case 1
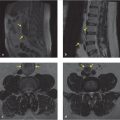
Case 1 demonstrates enlarged iliac chain lymph nodes incidentally detected at sacral MRI. Review of the patient’s prior CT demonstrates that these nodes have been stable (▶ Fig. 39.2). Given the stability over 1 year, this is considered a benign finding and no further follow-up is required.
Fig. 39.2 Axial CT images approximately a year earlier showed stable size of the lymph nodes (arrows). There was no history of malignancy or other condition that might cause the lymph node enlargement.
39.2 Case 2
39.2.1 History
A 67-year-old man presents with worsening back pain and known history of lung cancer.
39.2.2 Most Likely Imaging Diagnosis for Case 2
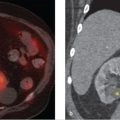
Case 2 demonstrates retroperitoneal adenopathy in the setting of disseminated metastatic disease.
Fig. 39.3 T2-weighted sagittal image (a) demonstrates enlarged para-aortic lymph nodes only seen on sagittal images (long arrows). Also note the bone metastasis in the T12 pedicle (short arrow). Axial T2-weighted image (b) demonstrates bilateral adrenal masses (arrows) in keeping with the patient’s known metastatic disease.
Differential diagnosis and imaging pitfalls
Comments
Metastatic disease/lymphoma
Lymphoma is often symmetric and will displace adjacent vascular structures (aorta, inferior vena cava [IVC]). Metastases tend to be more asymmetric and heterogeneous and there may be a known history of primary malignancy
Sarcoma
Liposarcoma is the most common sarcoma in the retroperitoneum. Look for areas of fat signal or fat attenuation within the large retroperitoneal mass
Retroperitoneal hemorrhage
May be due to underlying coagulopathy or ruptured aortic aneurysm High-attenuation fluid dissects along the fascial planes
IVC duplication/anomalies or collateral vessels
Tubular in shape like a vessel; flow voids or venous enhancement pattern may be visible
Retroperitoneal fibrosis
Ill-defined mass or soft-tissue thickening encasing lower aorta, IVC, and ureters without displacement or mass effect. However, it often causes medial ureteral deviation and obstruction
Only gold members can continue reading. Log In or Register to continue